
Sarcoma de Kaposi favorece o diagnóstico de doença de Castleman em paciente vivendo com HIV
DOI:
https://doi.org/10.5935/2764-734X.e20230325-ptPalavras-chave:
Sarcoma de Kaposi, Herpesvirus humano 8, HIV, Hiperplasia do linfonodo gigante, Relato de casoResumo
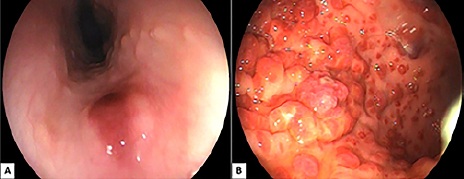
O herpesvírus humano 8 (HHV-8) é um vírus com capacidade de causar doença em pacientes imunodeprimidos, particularmente em indivíduos coinfectados pelo vírus da imunodeficiência humana (HIV). Algumas destas manifestações, como a doença de Castleman, são pouco comuns e o diagnóstico pode ser difícil pela variedade de sintomas inespecíficos e pela existência de múltiplos diagnósticos diferenciais. Reportamos o caso de um paciente vivendo com HIV cujo diagnóstico de doença de Castleman multicêntrica foi favorecido pela existência concomitante de sarcoma de Kaposi no trato gastrointestinal, lembrando que ambas entidades estão diretamente relacionadas à infecção pelo HHV-8.
Downloads
Referências
1. Chang Y, Cesarman E, Pessin MS, Lee F, Culpepper J, Knowles DM, et al. Identification of herpesvirus-like DNA sequences in AIDS-associated Kaposi’s sarcoma. Science. 1994 Dez;266(5192):1865-9.
2. Cesarman E, Chang Y, Moore PS, Said JW, Knowles DM. Kaposi’s sarcoma-associated herpesvirus-like DNA sequences in AIDS-related body-cavity-based
3. Soulier J, Grollet L, Oksenhendler E, Cacoub P, Cazals-Hatem D, Babinet P, et al. Kaposi’s sarcoma-associated herpesvirus-like DNA sequences in multicentric Castleman’s disease. Blood. 1995 Ago;86(4):1276-80.
4. Jordan MB, Allen CE, Weitzman S, Filipovich AH, McClain KL. How I treat hemophagocytic lymphohistiocytosis. Blood. 2011 Out;118(15):4041-52.
5. Freitas RB, Freitas MR, Linhares AC. Prevalence of human herpesvirus 8 antibodies in the population of Belém, Pará, Brazil. Rev Inst Med Trop S Paulo. 2002 Dez;44(6):309-13.
6. Biggar RJ, Whitby D, Marshall V, Linhares AC, Black F. Human herpesvirus 8 in Brazilian Amerindians: a hyperendemic population with a new subtype. J Infect Dis. 2000 Mai;181(5):1562-8.
7. Martin JN, Ganem DE, Osmond DH, Page-Shafer KA, Macrae D, Kedes DH. Sexual transmission and the natural history of human herpesvirus 8 infection. N Engl J Med. 1998 Abr;338(14):948-54.
8. Plancoulaine S, Abel L, Van Beveren M, Tregouet DA, Joubert M, Tortevoye P, et al. Human herpesvirus 8 transmission from mother to child and between siblings in an endemic population. Lancet. 2000 Set/Out;356(9235):1062-5.
9. Andreoni M, Sarmati L, Nicastri E, El Sawaf G, El Zalabani M, Uccella I, et al. Primary human herpesvirus 8 infection in immunocompetent children. JAMA. 2002 Mar;287(10):1295-3000.
10. Hengge UR, Ruzicka T, Tyring SK, Stuschke M, Roggendorf M, Schwartz RA, et al. Update on Kaposi’s sarcoma and other HHV8 associated diseases. Part 1: epidemiology, environmental predispositions, clinical manifestations, and therapy. Lancet Infect Dis. 2002 Mai;2(5):281-92.
11. Engels EA, Pfeiffer RM, Goedert JJ, Virgo P, McNeel TS, Scoppa SM, et al. Trends in cancer risk among people with AIDS in the United States 1980-2002. AIDS. 2006 Ago;20(12):1645-54.
12. Castleman B, Iverson L, Menendez VP. Localized mediastinal lymphnode hyperplasia resembling thymoma. Cancer. 1956 Jul;9(4):822-30.
13. Gaba AR, Stein RS, Sweet DL, Variakojis D. Multicentric giant lymph node hyperplasia. Am J Clin Pathol. 1978 Jan;69(1):86-90.
14. Bower M, Newsom-Davis T, Naresh K, Merchant S, Lee B, Gazzard B, et al. Clinical features and outcome in HIV-associated multicentric Castleman’s disease. J Clin Oncol. 2011 Jun;29(18):2481-6.
15. Collins LS, Fowler A, Tong CY, Ruiter A. Multicentric Castleman’s disease in HIV infection. Int J STD AIDS. 2006 Jan;17(1):19-24;quiz:5.
16. Guihot A, Couderc LJ, Rivaud E, Galicier L, Bossi P, Oksenhendler E, et al. Thoracic radiographic and CT findings of multicentric Castleman disease in HIV-infected patients. J Thorac Imaging. 2007 Mai;22(2):207-11.
17. Dupin N, Diss TL, Kellam P, Tulliez M, Du MQ, Sicard D, et al. HHV-8 is associated with a plasmablastic variant of Castleman disease that is linked to HHV-8-positive plasmablastic lymphoma. Blood. 2000 Fev;95(4):1406-12.
18. Ramaswami R, Lurain K, Polizzotto MN, Ekwede I, Waldon K, Steinberg SM, et al. Characteristics and outcomes of KSHV-associated multicentric Castleman disease with or without other KSHV diseases. Blood Adv. 2021 Mar;5(6):1660-70.
19. Uldrick TS, Polizzotto MN, Aleman K, Wyvill KM, Marshall V, Whitby D, et al. Rituximab plus liposomal doxorubicin in HIV-infected patients with KSHV-associated multicentric Castleman disease. Blood. 2014 Dez;124(24):3544-52.
20. Uldrick TS, Wang V, O’Mahony D, Aleman K, Wyvill KM, Marshall V, et al. An interleukin-6-related systemic inflammatory syndrome in patients co-infected with Kaposi sarcoma-associated herpesvirus and HIV but without Multicentric Castleman disease. Clin Infect Dis. 2010 Ago;51(3):350-8.
21. Polizzotto MN, Uldrick TS, Wyvill KM, Aleman K, Marshall V, Wang V, et al. Clinical features and outcomes of patients with symptomatic Kaposi Sarcoma Herpesvirus (KSHV)-associated inflammation: prospective characterization of KSHV Inflammatory Cytokine Syndrome (KICS). Clin Infect Dis. 2016 Mar;62(6):730-8.
22. Filipovich A, McClain K, Grom A. Histiocytic disorders: recent insights into pathophysiology and practical guidelines. Biol Blood Marrow Transplant. 2010 Jan;16(Supl 1):S82-S9.
Downloads
Publicado
Como Citar
Edição
Seção
Licença
Copyright (c) 2023 Infectologia em Evidência

Este trabalho está licenciado sob uma licença Creative Commons Attribution 4.0 International License.
Todos os usuários podem ler, baixar, compartilhar e adaptar esta produção científica livremente para quaisquer fins (mesmo que comerciais), desde que seja dado o devido crédito aos autores e à publicação original e que qualquer alteração seja devidamente indicada.
> Ética
Todos os artigos publicados na Revista gozam de uma aprovação ética do Sistema Nacional de Ética em Pesquisa (antigo sistema CEP/CONEP) com base na Lei Federal 14.874/24 e outras regulamentações específicas brasileiras ou documento semelhante atestando a ciência e autorização por parte da instituição de origem no caso de trabalhos estrangeiros.
Os autores declaram não haver nenhum tipo de patrocínio ou conflito de interesses, salvo indicação em contrário no corpo do artigo.
Vale ressaltar que os relatos de caso são um valioso recurso de aprendizado para a comunidade científica, mas não devem ser utilizados isoladamente para guiar opções diagnósticas ou terapêuticas na prática clínica ou em políticas de saúde.








