

Mielite transversa pelo vírus varicela-zoster na ausência de lesões cutâneas
DOI:
https://doi.org/10.5935/2764-734X.e20231231Palavras-chave:
Infecção pelo vírus da varicela-zoster, Mielite transversa, Zoster sine herpete, Relato de casoResumo
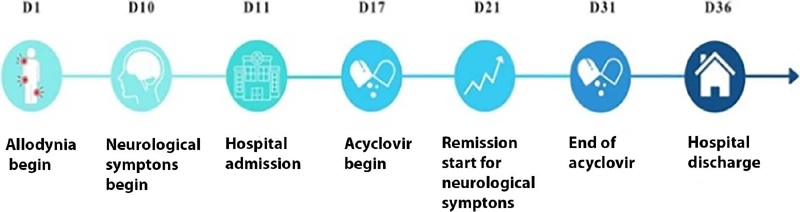
A mielite pelo vírus varicela-zoster (VZV) é uma complicação rara em indivíduos sem disfunção imunológica, porém relativamente frequente em imunocomprometidos. As alterações neurológicas podem ser graves e levar ao óbito ou resultar em sequelas, principalmente se houver atraso para o início do tratamento. Relatamos o caso clínico de uma mulher trans, infectada pelo vírus HIV com queixa de retenção urinária, paresia e parestesia de membros inferiores depois de 10 dias do aparecimento de alodínia em um dermátomo torácico acometido por herpes zoster no passado. Não havia qualquer outra lesão cutânea como as vesículas e bolhas típicas da reativação do VZV e os exames complementares todos não foram capazes de estabelecer um diagnóstico etiológico inequívoco. Mesmo assim, o tratamento empírico com aciclovir endovenoso em altas doses por 14 dias apresentou boa resposta clínica, com imediata reversão parcial dos déficits neurológicos.
Downloads
Referências
1. Moshayedi P, Thomas D, Rinaldo CR, Moossy JJ, Maroon JC, Murdoch GH, et al. Subacute histopathological features in a case of varicella zoster virus myelitis and post-herpetic neuralgia. Spinal Cord Ser Cases. 2018 Apr;4(1):33. DOI: 10.1038/s41394-018-0068-5
2. Lameiras C, Patrocínio de Jesus R, Flor-de-Lima B, Silva J, Pacheco P. A case of varicella-zoster virus meningomyelitis in an HIV-1-infected patient: facing the challenges related to its management and prognosis. Cureus. 2022 Aug;14(8):e27652. DOI: 10.7759/cureus.27652
3. Liu Q, Zhou X, Li Z. Acute myelitis with multicranial neuritis caused by varicella zoster virus: a case report. BMC Neurol. 2022;22(1):45. DOI: 10.1186/s12883-022-02571-y
4. Yun D, Cho SY, Ju W, Seo EH. Transverse myelitis after infection with varicella zoster virus in patient with normal immunity: a case report. World J Clin Cases. 2021 Nov;9(33):10308-14. DOI: 10.12998/wjcc.v9.i33.10308
5. Cree BAC. Acute inflammatory myelopathies. Handb Clin Neurol. 2014;122:613-67. DOI: 10.1016/B978-0-444-52001-2.00027-3
6. Simone CG, Emmady PD. Transverse Myelitis. [Updated 2022 Nov 15]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Disponível em: https://www.ncbi.nlm.nih.gov/books/NBK559302/
7. West TW. Transverse myelitis - a review of the presentation, diagnosis, and initial management. Discov Med. 2013;16(88):167-77. Disponível em: https://pubmed.ncbi.nlm.nih.gov/24099672/
8. Miyake Z, Tomidokoro Y, Nohara S, Tamaoka A. Chronic myelitis associated with zoster sine herpete. A case report. Medicine. 2019 Aug;98(32):e16671. DOI: 0.1097/MD.0000000000016671
9. Blanchardiere AD, Rozenberg F, Caumes E, O Picard, F Lionnet, J Livartowski, et al. Neurological complications of varicella-zoster virus infection in adults with human immunodeficiency virus infection. Scand J Dis. 2000;32(3):263-9. DOI: 10.1080/00365540050165893
10. Zhou J, Li J, Ma L, Cao S. Zoster sine herpete: a review. Korean J Pain. 2020 Jul;33(3):208-15. DOI: 10.3344/kjp.2020.33.3.208
11. Takahashi T, Tamura M, Miki K, Yamaguchi M, Kanno A, Nunomura S, et al. Varicella zoster virus myelitis in two elderly patients: diagnostic value of nested polymerase chain reaction assay and antibody index for cerebrospinal fluid specimens. Case Rep Neurol. 2013 Apr;5(1):81-90. DOI: 10.1159/000350714
Downloads
Publicado
Como Citar
Edição
Seção
Licença
Copyright (c) 2023 Infectologia em Evidência

Este trabalho está licenciado sob uma licença Creative Commons Attribution 4.0 International License.
Todos os usuários podem ler, baixar, compartilhar e adaptar esta produção científica livremente para quaisquer fins (mesmo que comerciais), desde que seja dado o devido crédito aos autores e à publicação original e que qualquer alteração seja devidamente indicada.
> Ética
Todos os artigos publicados na Revista gozam de uma aprovação ética do Sistema Nacional de Ética em Pesquisa (antigo sistema CEP/CONEP) com base na Lei Federal 14.874/24 e outras regulamentações específicas brasileiras ou documento semelhante atestando a ciência e autorização por parte da instituição de origem no caso de trabalhos estrangeiros.
Os autores declaram não haver nenhum tipo de patrocínio ou conflito de interesses, salvo indicação em contrário no corpo do artigo.
Vale ressaltar que os relatos de caso são um valioso recurso de aprendizado para a comunidade científica, mas não devem ser utilizados isoladamente para guiar opções diagnósticas ou terapêuticas na prática clínica ou em políticas de saúde.








