
Rabdomiólise secundária à infecção pelo vírus Influenza
DOI:
https://doi.org/10.5935/2764-734X.e20240139Palavras-chave:
Influenza humana, Rabdomiólise, Vírus da influenza A subtipo H1N1, Creatina quinase, Relato de casoResumo
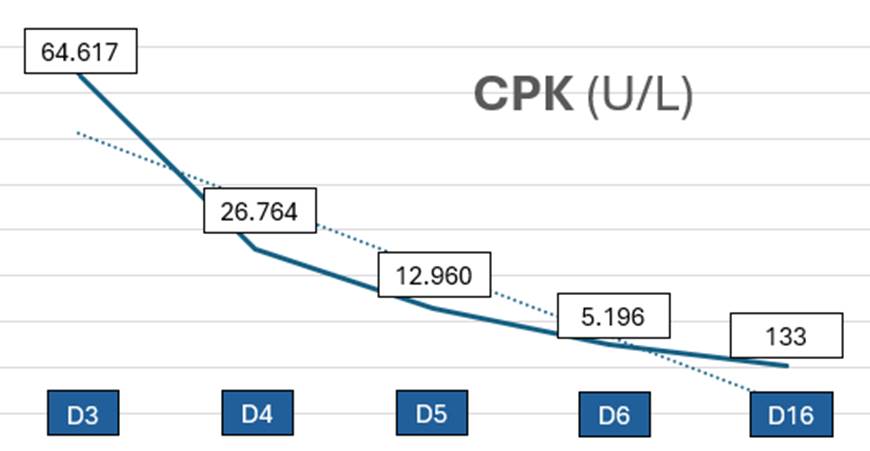
A rabdomiólise é uma condição potencialmente grave que pode resultar, dentre outros, da infecção por Influenza. Relatamos o caso de um jovem de 32 anos, sem comorbidades, o qual apresentou febre, mialgia e urina escurecida há quatro dias, seguidas de tosse e coriza. Os exames mostraram elevação significativa da creatinofosfoquinase (64.617U/L) e das transaminases. As principais hipóteses diagnósticas para justificar o quadro foram de etiologia infecciosa, em especial a leptospirose e hepatite viral aguda, antes da confirmação específica da infecção por Influenza A e B. Além de ter sido medicado com ceftriaxona por 10 dias, o paciente recebeu vigorosa e precoce hidratação intravenosa – fator que contribuiu, com certeza, para a boa evolução clínica e laboratorial, sem desenvolver lesão renal.
Downloads
Referências
1. Torres PA, Helmstetter JA, Kaye AM, Kaye AD. Rhabdomyolysis: pathogenesis, diagnosis, and treatment. Ochsner J. 2015;15(1):58-69. Disponível em: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4365849/
2. Fadila MF, Wool KJ. Rhabdomyolysis secondary to influenza a infection: a case report and review of the literature. N Am J Med Sci. 2015;7(3):122-4. DOI: https://doi.org/10.4103/1947-2714.153926
3. Singh U, Scheld WM. Infectious etiologies of rhabdomyolysis: three case reports and review. Clin Infect Dis. 1996;22(4):642-9. DOI: 10.1093/clinids/22.4.642
4. Paules C, Subbarao K. Influenza. Lancet. 2017;390(10095):697-708. DOI: 10.1016/S0140-6736(17)30129-0
5. Krammer F, Smith GJD, Fouchier RAM, Peiris M, Kedzierska K, Doherty PC, et al. Influenza. Nat Rev Dis Primers. 2018;4(1):3. DOI: 10.1038/s41572-018-0002-y
6. Almeida ARM. Dinâmica sazonal da influenza no Brasil: a importância da latitude e do clima [Tese na Internet]. Rio de Janeiro: Escola Nacional de Saúde Pública Sergio Arouca (ENSP)/Fundação Oswaldo Cruz (FIOCRUZ); 2018; [acesso em 2023 Out 10]. Disponível em: https://www.arca.fiocruz.br/bitstream/handle/icict/34080/ve_Alexandra_Ribeiro_ENSP_2018?sequence=2&isAllowed=y
7. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância em Saúde e Ambiente. Informe Técnico Operacional: Vacinação contra a Influenza [Internet]. 1ª ed. Brasília: Ministério da Saúde; 2023; [acesso em 2024 Jan 31]. Disponível em: https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/c/cale8ndario-nacional-de-vacinacao/arquivos/informe-tecnico-operacional-de-vacinacao-contra-a-influenza-2023
8. Nicholls JM, Chan RW, Russell RJ, Air GM, Peiris JS. Evolving complexities of influenza virus and its receptors. Trends Microbiol. 2008;16(4):149-57. DOI: 10.1016/j.tim.2008.01.008
9. Desdouits M, Munier S, Prevost MC, Jeannin P, Butler-Browne G, Ozden S, et al. Productive infection of human skeletal muscle cells by pandemic and seasonal influenza A(H1N1) viruses. PLoS One. 2013;8(11):e79628. DOI: 10.1371/journal.pone.0079628
10. Tanaka T, Takada T, Takagi D, Takeyama N, Kitazawa Y. Acute renal failure due to rhabdomyolysis associated with echovirus 9 infection: a case report and review of literature. Jpn J Med. 1989;28(2):237-42. DOI: 10.2169/internalmedicine1962.28.237
11. Perez-Padilla R, de la Rosa-Zamboni D, Ponce de Leon S, Hernandez M, Quiñones-Falconi F, Bautista E, et al. Pneumonia and respiratory failure from swine-origin influenza A (H1N1) in Mexico. N Engl J Med. 2009;361(7):680-9. DOI: 10.1056/NEJMoa0904252
12. Borgatta B, Pérez M, Rello J, Vidaur L, Lorente L, Socías L, et al. Elevation of creatine kinase is associated with worse outcomes in 2009 pH1N1 influenza A infection. Intensive Care Med. 2012;38(7):1152-61. DOI: 10.1007/s00134-012-2565-5
13. Runnstrom M, Ebied AM, Khoury AP, Reddy R. Influenza-induced rhabdomyolysis. BMJ Case Rep. 2018;11(1):e226610. DOI: 10.1136/bcr-2018-226610
14. Sato E, Nakamura T, Koide H. Rhabdomyolysis induced by influenza A infection: case report and review of literature. Ther Apher Dial. 2011;15(2):208-9. DOI: 10.1111/j.1744-9987.2010.00900.x
15. Lai CC, Wang CY, Lin HI. Rhabdomyolysis and acute kidney injury associated with 2009 pandemic influenza A(H1N1). Am J Kidney Dis. 2010;55(3):615. DOI: 10.1053/j.ajkd.2010.01.002
16. Uyeki TM, Bernstein HH, Bradley JS, Englund JA, File TM, Fry AM, et al. clinical practice guidelines by the Infectious Diseases Society of America: 2018 update on diagnosis, treatment, chemoprophylaxis, and institutional outbreak management of seasonal Influenza. Clin Infect Dis. 2019;68(6):895-902. DOI: 10.1093/cid/ciy874
Downloads
Publicado
Como Citar
Edição
Seção
Licença
Copyright (c) 2025 Infectologia em Evidência

Este trabalho está licenciado sob uma licença Creative Commons Attribution 4.0 International License.
Todos os usuários podem ler, baixar, compartilhar e adaptar esta produção científica livremente para quaisquer fins (mesmo que comerciais), desde que seja dado o devido crédito aos autores e à publicação original e que qualquer alteração seja devidamente indicada.
> Ética
Todos os artigos publicados na Revista gozam de uma aprovação ética do Sistema Nacional de Ética em Pesquisa (antigo sistema CEP/CONEP) com base na Lei Federal 14.874/24 e outras regulamentações específicas brasileiras ou documento semelhante atestando a ciência e autorização por parte da instituição de origem no caso de trabalhos estrangeiros.
Os autores declaram não haver nenhum tipo de patrocínio ou conflito de interesses, salvo indicação em contrário no corpo do artigo.
Vale ressaltar que os relatos de caso são um valioso recurso de aprendizado para a comunidade científica, mas não devem ser utilizados isoladamente para guiar opções diagnósticas ou terapêuticas na prática clínica ou em políticas de saúde.








