
Otomastoidite: forma rara de tuberculose extra-pulmonar
DOI:
https://doi.org/10.5935/2764-734X.e20240946Palavras-chave:
Tuberculose Extrapulmonar, Otite Média Supurativa, Tuberculose Pulmonar, Mastoidite, Relato de CasoResumo
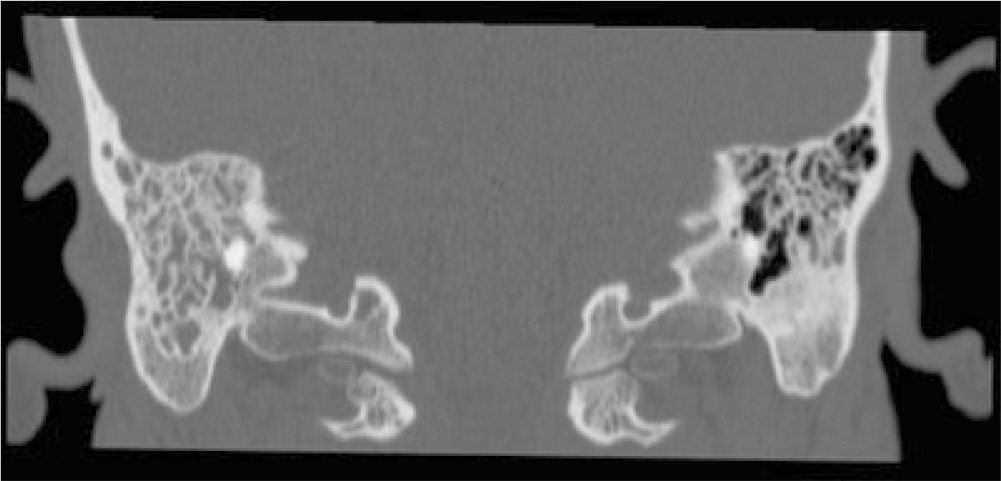
Apesar de predominantemente associada a manifestações pulmonares, a otite média tuberculosa é uma manifestação clínica rara da disseminação extrapulmonar da infecção. Este relato de caso apresenta um paciente de 41 anos infectado por HIV/aids que, 10 dias depois de ter sido agredido fisicamente, evoluiu com otalgia, otorreia, tosse, dispneia e perda de peso. Foi admitido com sepse por foco pulmonar, todavia foi identificada a presença de Mycobacterium tuberculosis no escarro através de teste rápido molecular, já no segundo dia de internação. A tomografia computadorizada de crânio revelou mastoidite à direita (sem lesão óssea) e a secreção do ouvido também confirmou a etiologia tuberculosa. Houve boa resposta ao tratamento específico.
Downloads
Referências
1. World Health Organization (WHO). Global tuberculosis report 2023 [Internet]. Geneva: WHO; 2023; [acesso em 2024 Mai 25]. Disponível em: https://iris.who.int/bitstream/handle/10665/373828/9789240083851-eng.pdf?sequence=1
2. Pai KK, Omiunu AO, Peddu DK, Au VH, Baredes S, Jyung RW, et al. Tuberculosis of the middle ear: a systematic review. Am J Otolaryngol. 2022;43(5):103571. DOI: 10.1016/j.amjoto.2022.103571
3. Cao T, Liu X, Yang C, Mei C, Ou J, Du R. Multidrug-resistant tuberculosis in middle ear: a case report. J Clin Tuberc Other Mycobact Dis. 2023;31:100355. DOI: 10.1016/j.jctube.2023.100355
4. Deenadayal DS, Kumar BN, Bommakanti V, Sameeri KL. Tuberculous otitis media - a rare entity or a missed diagnosis. Int J Otolaryngol Head Neck Surg. 2016;5(02):65. DOI: 10.4236/ijohns.2016.52011
5. Sens PM, Almeida CI, Valle LO, Costa LH, Angeli ML. Tuberculosis of the ear, a professional disease? Braz J Otorhinolaryngol. 2008;74(4):621-7. DOI: 10.1016/s1808-8694(15)30614-5
6. Saunders NC, Albert DM. Tuberculous mastoiditis: When is surgery indicated? Int J Pediatr Otorhinolaryngol. 2002;65(1):59-63. DOI: 10.1016/s0165-5876(02)00121-0
7. Singh A, Irugu DV, Verma H, Thakar A. Atypical presentation of aural tuberculosis with complication. BMJ Case Rep. 2018;2018:bcr-2017-222482. DOI: 10.1136/bcr-2017-222482
8. Dale OT, Clarke AR, Drysdale AJ. Challenges encountered in the diagnosis of tuberculous otitis media: case report and literature review. J Laryngol Otol. 2011;125(7):738-40. DOI: 10.1017/S0022215111000971
9. Sebastian SK, Singhal A, Sharma A, Doloi P. Tuberculous otitis media - series of 10 cases. J Otology. 2020;15(3):95-8. DOI: 10.1016/j.joto.2019.12.001
10. Salata TM, Ribeiro BN, Muniz BC, Antunes LO, Rosas HB, Marchiori E. Distúrbios da audição - achados na tomografia computadorizada e ressonância magnética: ensaio iconográfico. Radiol Bras. 2018;52:54-9. DOI: 10.1590/0100-3984.2016.0213
11. Rubio JMD, Alarcon AV, Palma DM, Vales O, Hinojosa R, Morales DJ, et al. Neuro-otologic manifestations of tuberculosis: "the great imitator." Am J Otolaryngol. 2015;36(3):467-71. DOI: 10.1016/j.amjoto.2015.01.018
Downloads
Publicado
Como Citar
Edição
Seção
Licença
Copyright (c) 2025 Infectologia em Evidência

Este trabalho está licenciado sob uma licença Creative Commons Attribution 4.0 International License.
Todos os usuários podem ler, baixar, compartilhar e adaptar esta produção científica livremente para quaisquer fins (mesmo que comerciais), desde que seja dado o devido crédito aos autores e à publicação original e que qualquer alteração seja devidamente indicada.
> Ética
Todos os artigos publicados na Revista gozam de uma aprovação ética do Sistema Nacional de Ética em Pesquisa (antigo sistema CEP/CONEP) com base na Lei Federal 14.874/24 e outras regulamentações específicas brasileiras ou documento semelhante atestando a ciência e autorização por parte da instituição de origem no caso de trabalhos estrangeiros.
Os autores declaram não haver nenhum tipo de patrocínio ou conflito de interesses, salvo indicação em contrário no corpo do artigo.
Vale ressaltar que os relatos de caso são um valioso recurso de aprendizado para a comunidade científica, mas não devem ser utilizados isoladamente para guiar opções diagnósticas ou terapêuticas na prática clínica ou em políticas de saúde.








