
Lesões Osteolíticas em Paciente vivendo com HIV
DOI:
https://doi.org/10.5935/2764-734X.e20250353Palavras-chave:
Infecções oportunistas associadas à AIDS, Relato de Caso, Sarcoma de Kaposi, Tuberculose óssea, Herpesvírus Humano 8Resumo
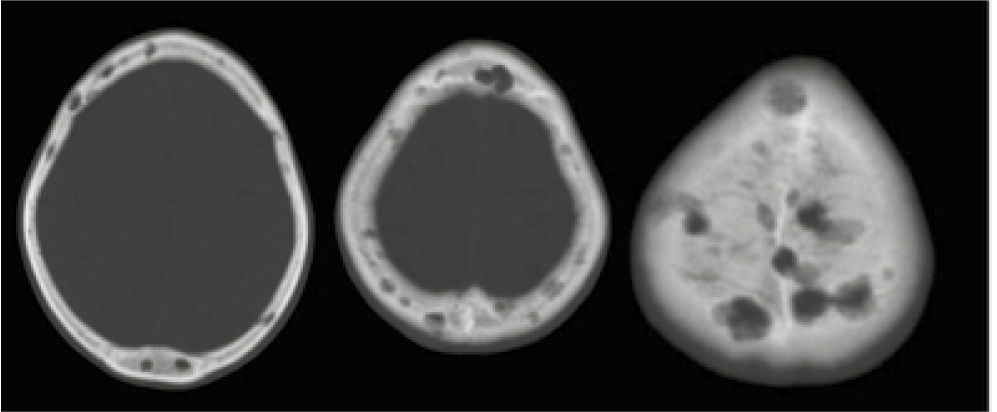
Este relato de caso descreve um paciente masculino de 22 anos infectado pelo HIV com queixa pulmonar e cutânea, cujas imagens tomográficas iniciais evidenciaram lesões líticas no esterno, escápula e corpos vertebrais, além da calota craniana, no osso ilíaco, sacro, úmero, tíbia e fêmur, de imediato levantando a suspeita de uma neoplasia metastática ou de mieloma múltiplo. Foi diagnosticada tuberculose pulmonar (com sensibilidade preservada à rifampicina) através do escarro, enquanto a biópsia da pele firmou o diagnóstico de sarcoma de Kaposi. A biópsia óssea do esterno, no entanto, foi inconclusiva: embora tenha afastado qualquer tipo de infiltração neoplásica, não foi possível confirmar tuberculose ou sarcoma naquela topografia. O paciente evadiu do hospital antes de se progredir a investigação rumo a um diagnóstico definitivo, porém uma breve revisão da literatura destaca a possibilidade de etiologias oportunistas originarem lesões osteolíticas em pacientes vivendo com HIV/aids.
Downloads
Referências
1. Clézardin P, Coleman R, Puppo M, Ottewell P, Bonnelye E, Paycha F, et al. Bone metastasis: mechanisms, therapies, and biomarkers. Physiol Rev. 2021 Jul 1;101(3):797-855. DOI: 10.1152/physrev.00012.2019
2. Subramanian S, Viswanathan VK. Lytic bone lesions. In: StatPearls [Internet]. Treasure Island: StatPearls Publishing; 2024. [Accessed 2024 Sep 10]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539837
3. Tehranzadeh J, Ter-Oganesyan RR, Steinbach LS. Musculoskeletal disorders associated with HIV infection and AIDS: Part I: infectious musculoskeletal conditions. Skeletal Radiol. 2004 May;33(5):249-59. DOI: 10.1007/s00256-004-0764-z
4. Rajkumar SV. Multiple myeloma: 2024 update on diagnosis, risk-stratification, and management. Am J Hematol. 2024 Sep;99(9):1802-24. DOI: 10.1002/ajh.27422
5. Yergiyev O, Mohanty A, Curran-Melendez S, Latona CR, Bhagavatula R, Greenberg L, et al. Fine-needle aspiration cytology of disseminated Kaposi sarcoma of the bone in an AIDS patient. Acta Cytol. 2015;59(1):113- 7. DOI: 10.1159/000369855
6. Thanos L, Mylona S, Kalioras V, Pomoni M, Batakis N. Osseous Kaposi sarcoma in an HIV-positive patient. Skeletal Radiol. 2004 Apr;33(4):241-3. DOI: 10.1007/s00256-003-0732-z
7. Caponetti G, Dezube BJ, Restrepo CS, Pantanowitz L. Kaposi sarcoma of the musculoskeletal system: a review of 66 patients. Cancer. 2007 Mar 15;109(6):1040-52. DOI: 10.1002/cncr.22500
8. Bell BM Jr, Syed A, Carmack SW, Thomas CA, Layton KF. Disseminated Kaposi sarcoma with osseous metastases in an HIV-positive patient. Proc (Bayl Univ Med Cent). 2016 Jan;29(1):52-4. DOI: 10.1080/08998280.2016.11929358
9. Hodkinson B, Osman N, Botha-Scheepers S. HIV Infection and Osteoarticular Tuberculosis: Strange Bedfellows. Case Rep Rheumatol. 2016;2016:5718423. DOI: 10.1155/2016/5718423
10. Pigrau-Serrallach C, Rodríguez-Pardo D. Bone and joint tuberculosis. Eur Spine J. 2013 Jun;22(Suppl 4):556-66. DOI: 10.1007/s00586-012-2331-y
11. Shiels MS, Althoff KN, Pfeiffer RM, Achenbach CJ, Abraham AG, Castilho J, et al. Engels EA; North American AIDS Cohort Collaboration on Research and Design (NA-ACCORD) of the International Epidemiologic Databases to Evaluate AIDS (IeDEA). HIV Infection, Immunosuppression, and Age at Diagnosis of Non - AIDS-Defining Cancers. Clin Infect Dis. 2017 Feb 15;64(4):468-75. DOI:10.1016/S2352-3018(20)30118-1
12. De Groot JJB, Webb MJ, Raubenheimer JE, Struwig MC, Louw VJ. Concomitant HIV infection in newly diagnosed multiple myeloma patients is hard to recognise and should be tested for routinely in areas of high endemicity. S Afr Med J. 2017 Aug 25;107(9):781-7. DOI:10.7196/SAMJ.2017.v107i9.12360
13. Connolly SP, McGrath J, Sui J, Muldoon EG. Rare, disseminated Kaposi sarcoma in advanced HIV with high-burden pulmonary and skeletal involvement. Rare, disseminated Kaposi sarcoma in advanced HIV with high-burden pulmonary and skeletal involvement. BMJ Case Rep. 2021 Dec 1;14(12):e245448. DOI: 10.1136/bcr-2021-245448
14. Mellat-Ardakani M, Ghiasvand F, Nezhad MH, Salahshour F, SeyedAlinaghi S. Multifocal Osteolytic Lesions in Skull Bone with Mycobacterium Tuberculosis: A Case Report. Infect Disord Drug Targets. 2021;21(5):e270421187878. DOI: 10.2174/18715265 20999201111200140
15. Colquhoun M, Kirresh O, Keikha M, Haddow L. Osteolytic lesions as the sole presenting feature of secondary syphilis. BMJ Case Rep. 2021 Jun 22;14(6):e242814. DOI:10.1136/bcr-2021242814
16. Park KH, Lee MS, Hong IK, Sung JY, Choi SH, Park SO, et al. Bone involvement in secondary syphilis: a case report and systematic review of the literature. Sex Transm Dis. 2014 Sep;41(9):532-7. DOI: 10.1097/OLQ.0000000000000164
17. Braekeveld P, Verstraete K, Deprest K, Van Hecke E, Kunnen M. Bacillary Angiomatosis in a Patient with AIDS - case 1717 [Internet]. EURORAD 2022 (8 oct). Accessed in 2025 January 10. Available from: www.eurorad.org/case/1717. DOI: 10.1594/EURORAD/CASE.1717
18. Baron AL, Steinbach LS, LeBoit PE, Mills CM, Gee JH, Berger TG. Osteolytic lesions and bacillary angiomatosis in HIV infection: radiologic differentiation from AIDS-related Kaposi sarcoma. Radiology. 1990 Oct;177(1):77-81. DOI: 10.1148/radiology.177.1.2399342
19. Murugan S. Multiple osteolytic lesions in a 14-year-old boy with HIV disease. Indian J Sex Transm Dis AIDS. 2015 Jan/Jun;36(1):92-4. DOI: 10.4103/2589-0557.156747
Downloads
Publicado
Como Citar
Edição
Seção
Licença
Copyright (c) 2025 Infectologia em Evidência

Este trabalho está licenciado sob uma licença Creative Commons Attribution 4.0 International License.
Todos os usuários podem ler, baixar, compartilhar e adaptar esta produção científica livremente para quaisquer fins (mesmo que comerciais), desde que seja dado o devido crédito aos autores e à publicação original e que qualquer alteração seja devidamente indicada.
> Ética
Todos os artigos publicados na Revista gozam de uma aprovação ética do Sistema Nacional de Ética em Pesquisa (antigo sistema CEP/CONEP) com base na Lei Federal 14.874/24 e outras regulamentações específicas brasileiras ou documento semelhante atestando a ciência e autorização por parte da instituição de origem no caso de trabalhos estrangeiros.
Os autores declaram não haver nenhum tipo de patrocínio ou conflito de interesses, salvo indicação em contrário no corpo do artigo.
Vale ressaltar que os relatos de caso são um valioso recurso de aprendizado para a comunidade científica, mas não devem ser utilizados isoladamente para guiar opções diagnósticas ou terapêuticas na prática clínica ou em políticas de saúde.








