
Lesão expansiva cerebral em paciente com aids
DOI:
https://doi.org/10.5935/2764-734X.e20250255Palavras-chave:
Infecções oportunistas relacionadas com a aids, Tuberculoma intracraniano, Toxoplasmose cerebral, Relato de CasoResumo
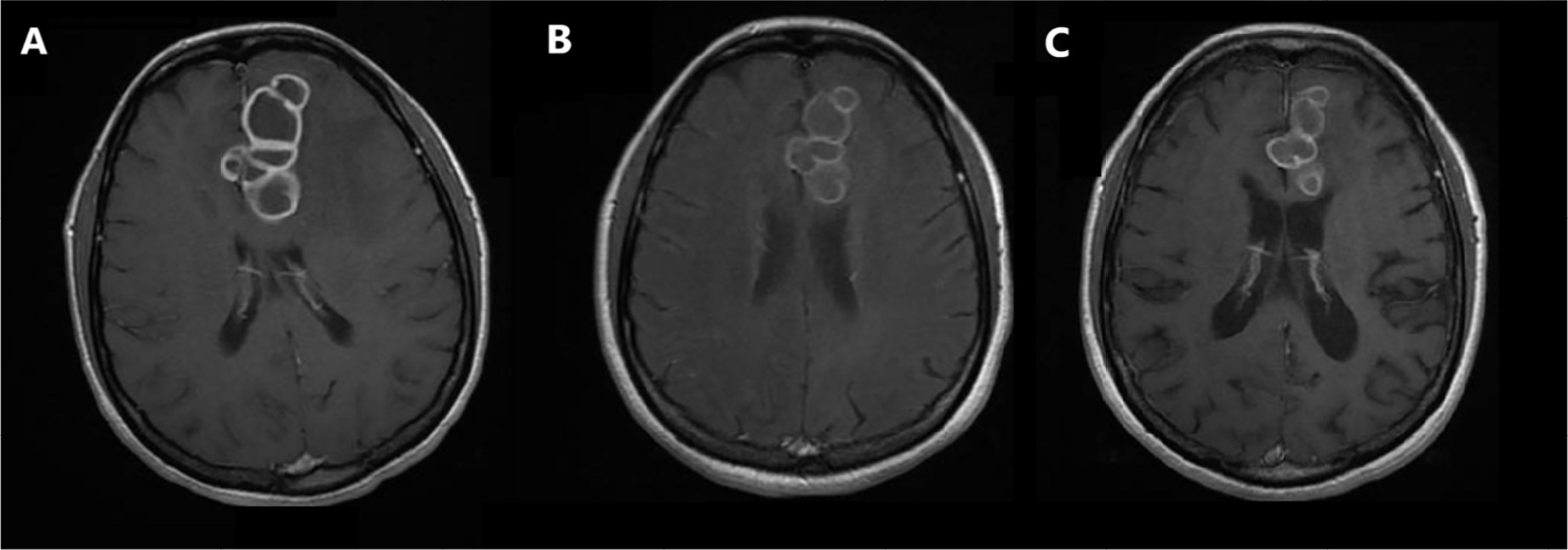
Os tuberculomas cerebrais constituem potenciais complicações da tuberculose disseminada em pessoas vivendo com o HIV/aids, principalmente nos países em desenvolvimento. Relatamos o caso de uma mulher de 52 anos com doença avançada pelo HIV e tuberculose pulmonar confirmada, a qual apresentou confusão mental, síncope e uma lesão tumoral intracraniana de aspecto multilobulado. Houve piora clínica e radiológica depois de três meses (já na fase de manutenção) do tratamento específico, fato que implicou em dúvidas terapêuticas, tendo a toxoplasmose cerebral como o principal diagnóstico diferencial, a ponto de também merecer tratamento empírico. Optou-se por reiniciar o esquema completo para tuberculose e associar corticosteróides. Uma segunda amostra de líquor exibiu bacilos ácido-álcool resistentes, mas a biópsia estereotáxica não identificou nenhum agente etiológico. Após uma internação prolongada de dois meses, a paciente recebeu alta hospitalar para seguimento ambulatorial, onde vem sendo acompanhada já por quase dois anos com melhora inequívoca do ponto de vista clínico, porém ainda parcial em relação às neuroimagens.
Downloads
Referências
1. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Manual de Recomendações para manejo da infecção pelo HIV em adultos. 1ª ed. Brasília: Ministério da Saúde; 2024. [Acesso 2025 fev 12]. Disponível em: https://www.gov.br/aids/pt-br/central-de-conteudo/pcdts/pcdt_hiv_modulo_1_2024.pdf
2. Vidal JE, Cimerman S, da Silva PR, Sztajnbok J, Coelho JF, Lins DL. Tuberculous brain abscess in a patient with AIDS: case report and literature review. Rev Inst Med Trop Sao Paulo. 2003 Mar-Apr;45(2):111-4. DOI: 10.1590/S0036-46652003000200013
3. Park M, Gupta RK. Central Nervous System Mycobacterium Infection: Tuberculosis and Beyond. Neuroimaging Clin N Am. 2023 Feb;33(1):105-24. DOI: 10.1016/j.nic.2022.07.006
4. Bernaerts A, Vanhoenacker FM, Parizel PM, Van Goethem JW, Van Altena R, Laridon A, et al. Tuberculosis of the central nervous system: overview of neuroradiological findings. Eur Radiol. 2003 Aug;13(8):1876-90. DOI: 10.1007/s00330-002-1608-7
5. Marais S, Pepper DJ, Marais BJ, Török ME. HIV-associated tuberculous meningitis--diagnostic and therapeutic challenges. Tuberculosis (Edinb). 2010 Nov;90(6):367-74. DOI: 10.1016/j.tube.2010.08.006
6. Parry AH, Wani AH, Shaheen FA, Wani AA, Feroz I, Ilyas M. Evaluation of intracranial tuberculomas using diffusion-weighted imaging (DWI), magnetic resonance spectroscopy (MRS) and susceptibility weighted imaging (SWI). Br J Radiol. 2018 Nov;91(1091):20180342. DOI: 10.1259/bjr.20180342
7. Goyal V, Elavarasi A, Abhishek, Shukla G, Behari M. Practice Trends in Treating Central Nervous System Tuberculosis and Outcomes at a Tertiary Care Hospital: A Cohort Study of 244 Cases. Ann Indian Acad Neurol. 2019 Jan-Mar;22(1):37-46. DOI: 10.4103/aian.AIAN_70_18
8. Vemula RC, Prasad BCM, Koyalmantham V, Hanu G. Role of Surgery in Intracranial Tuberculomas and Proposal of a Novel Diagnostic Criteria for Diagnosis (Sri Venkateswara Institute of Medical Sciences Criteria). World Neurosurg. 2020 Jun;138:e52-e65. DOI: 10.1016/j.wneu.2020.01.179
9. Nair BR, Rajshekhar V. Factors Predicting the Need for Prolonged (>24 Months) Antituberculous Treatment in Patients with Brain Tuberculomas. World Neurosurg. 2019 May;125:e236-e247. DOI: 10.1016/j.wneu.2019.01.053
10. Marais S, Van Toorn R, Chow FC, Manesh A, Siddiqi OK, Figaji A, et al; Tuberculous Meningitis International Research Consortium. Management of intracranial tuberculous mass lesions: how long should we treat for? Wellcome Open Res. 2019 Oct 31;4:158. DOI: 10.12688/wellcomeopenres.15501.2
11. Donovan J, Bang ND, Imran D, Nghia HDT, Burhan E, Huong DTT, et al; ACT HIV Investigators. Adjunctive Dexamethasone for Tuberculous Meningitis in HIV-Positive Adults. N Engl J Med. 2023 Oct 12;389(15):1357-67. DOI: 10.1056/NEJMoa2216218
12. Vidal JE, Cimerman S, Schiavon Nogueira R, Bonasser Filho F, Sztajnbok J, da Silva PR, et al. Paradoxical reaction during treatment of tuberculous brain abscess in a patient with AIDS. Rev Inst Med Trop Sao Paulo. 2003 May-Jun;45(3):177-8. DOI: 10.1590/S0036-46652003000300012
Downloads
Publicado
Como Citar
Edição
Seção
Licença
Copyright (c) 2025 Infectologia em Evidência

Este trabalho está licenciado sob uma licença Creative Commons Attribution 4.0 International License.
Todos os usuários podem ler, baixar, compartilhar e adaptar esta produção científica livremente para quaisquer fins (mesmo que comerciais), desde que seja dado o devido crédito aos autores e à publicação original e que qualquer alteração seja devidamente indicada.
> Ética
Todos os artigos publicados na Revista gozam de uma aprovação ética do Sistema Nacional de Ética em Pesquisa (antigo sistema CEP/CONEP) com base na Lei Federal 14.874/24 e outras regulamentações específicas brasileiras ou documento semelhante atestando a ciência e autorização por parte da instituição de origem no caso de trabalhos estrangeiros.
Os autores declaram não haver nenhum tipo de patrocínio ou conflito de interesses, salvo indicação em contrário no corpo do artigo.
Vale ressaltar que os relatos de caso são um valioso recurso de aprendizado para a comunidade científica, mas não devem ser utilizados isoladamente para guiar opções diagnósticas ou terapêuticas na prática clínica ou em políticas de saúde.








