
Nefrectomia por Proteus mirabilis em paciente sem sinal de sepse
DOI:
https://doi.org/10.5935/2764-734X.e202112005Palavras-chave:
Nefrolitíase, Proteus mirabilis, PionefroseResumo
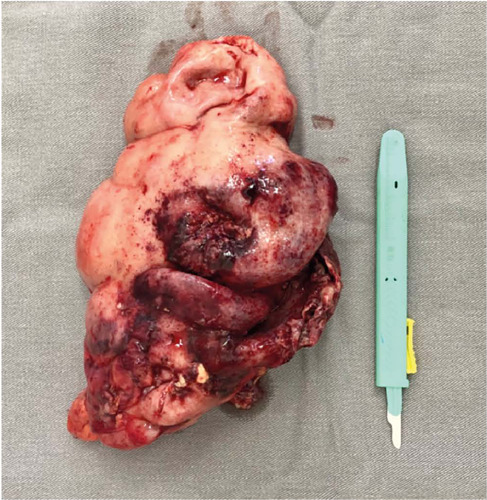
Mulher de 40 anos apresentava dor abdominal há 3 dias sem associação com sintomas urinários. Havia história de litíase renal não tratada há 6 anos. Ao exame físico não apresentava sinais de sepse, enquanto a tomografia computadorizada denotava destruição renal. Realizada nefrectomia com presença de Proteus mirabilis na cultura. Sabe-se que esta bactéria está associada à formação de cálculo de estruvita, podendo causar pionefrose. Infelizmente a paciente perdeu o rim devido a tratamento inadequado.
Downloads
Referências
1. Armbruster CE, Mobley HLT, Pearson MM. Pathogenesis of Proteus mirabilis infection. EcoSal Plus. 2018 Feb;8(1):ESP0009.
2. Mobley HLT. Proteus mirabilis overview. Methods Mol Biol. 2019;2021:1-4.
3. Pearson MM. Culture methods for Proteus mirabilis. Methods Mol Biol. 2019;2021:5-13.
4. Allison C, Emödy L, Coleman N, Hughes C. The role of swarm cell differentiation and multicellular migration in the uropathogenicity of Proteus mirabilis. J Infect Dis. 1994;169(5):1155-8.
5. Norsworthy AN, Pearson MM. From catheter to kidney stone: the uropathogenic lifestyle of Proteus mirabilis. Trends Microbiol. 2017 Apr;25(4):304-15.
6. Li X, Lockatell CV, Johnson DE, Lane MC, Warren JW, Mobley HLT. Development of an intranasal vaccine to prevent urinary tract infection by Proteus mirabilis. Infect Immun. 2004 Jan;72(1):66-75.
7. Quhal F, Seitz C. Guideline of the guidelines: urolithiasis. Curr Opin Urol. 2021 Mar;31(2):125-9.
8. Gupta K, Hooton TM, Naber KG, Wullt B, Colgan R, Miller LG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis. 2011 Mar;52(5):e103-20.
9. Xin J, Huang SD, Yu LX, Xin MH, Cai JS, Su ZJ. Pneumatic lithotripsy under ureteroscope for pyonephrosis due to calculus obstruction. Di Yi Jun Yi Da Xue Xue Bao. 2004 Oct;24(10):1199-20.
10. Jiang P, Xie L, Arada R, Patel RM, Landman J, Clayman RV. Qualitative review of clinical guidelines for medical and surgical management of urolithiasis: consensus and controversy 2020. J Urol. 2021 Apr;205(4):999-1008.
11. Romano J, Estrada C, Suárez N. Coraliform lithiasis. Aten Primaria. 2019 Aug/Sep;51(7):452-3.
12. Mahalingam H, Lal A, Mandal AK, Singh SK, Bhattacharyya S, Khandelwal N. Evaluation of low-dose dual energy computed tomography for in vivo assessment of renal/ureteric calculus composition. Korean J Urol. 2015 Aug;56(8):587-93.
13. Oka H, Nagamori T, Yamamoto S, Manabe H, Taketazu G, Mukai T, et al. Non-invasive discrimination of acute focal bacterial nephritis with pyelonephritis. Pediatr Int. 2019 Aug;61(8):777-80.
14. Chang CW, Huang CN. Pyonephrosis drained by double-J catheter. Clin Case Rep. 2020 Sep;8(12):3586-7.
15. Liu J, Chen L, An L, Ma K, Ye X, Xu Q, et al. Challenges and management of laparoscopic treatment of pyonephrosis caused by calculi. BMC Surg. 2020 Dec;20(1):327.
16. Florido C, Herren JL, Pandhi MB, Niemeyer MM. Emergent percutaneous nephrostomy for pyonephrosis: a primer for the on-call interventional radiologist. Semin Intervent Radiol. 2020 Mar;37(1):74-84.
Downloads
Publicado
Como Citar
Edição
Seção
Licença
Copyright (c) 2022 Infectologia em Evidência

Este trabalho está licenciado sob uma licença Creative Commons Attribution 4.0 International License.
Todos os usuários podem ler, baixar, compartilhar e adaptar esta produção científica livremente para quaisquer fins (mesmo que comerciais), desde que seja dado o devido crédito aos autores e à publicação original e que qualquer alteração seja devidamente indicada.
> Ética
Todos os artigos publicados na Revista gozam de uma aprovação ética do Sistema Nacional de Ética em Pesquisa (antigo sistema CEP/CONEP) com base na Lei Federal 14.874/24 e outras regulamentações específicas brasileiras ou documento semelhante atestando a ciência e autorização por parte da instituição de origem no caso de trabalhos estrangeiros.
Os autores declaram não haver nenhum tipo de patrocínio ou conflito de interesses, salvo indicação em contrário no corpo do artigo.
Vale ressaltar que os relatos de caso são um valioso recurso de aprendizado para a comunidade científica, mas não devem ser utilizados isoladamente para guiar opções diagnósticas ou terapêuticas na prática clínica ou em políticas de saúde.








