
Sífilis causando lesões ulceradas crostosas disseminadas em paciente imunossuprimido
DOI:
https://doi.org/10.5935/2764-734X.e202205011Palavras-chave:
Sífilis Cutânea, Síndrome de Imunodeficiência Adquirida, Verrugas, Relato de CasoResumo
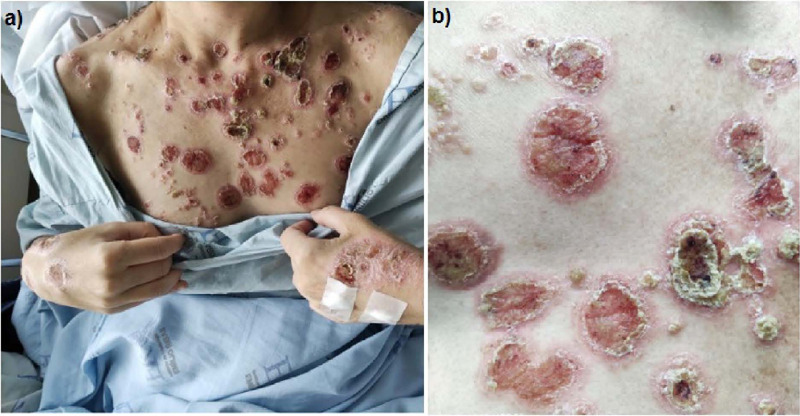
Indivíduos infectados pelo vírus da imunodeficiência humana (HIV) possuem maior risco de coinfecção com sífilis, podendo cursar com evolução diferente daqueles soronegativos, por vezes de forma mais rápida e agressiva. A manifestação de secundarismo é proporcionalmente mais prevalente, sendo a sífilis maligna (SM) uma forma rara deste estágio da doença, mas com expressivo aumento do número de casos após a epidemia de aids. A SM apresenta-se com lesões pleomórficas, descritas classicamente como úlcero-nodulares disseminadas, acompanhadas de sintomas constitucionais mais intensos. Este relato descreve o caso de uma paciente cujo diagnóstico de HIV foi simultâneo ao de sífilis recente, ocorrido durante investigação de lesões cutâneas disseminadas, ulceradas e crostosas, por vezes com aspecto rupióide. O diagnóstico de sífilis secundária foi estabelecido em associação a neurossífilis assintomática. Apesar dos critérios clínicos e laboratoriais compatíveis com o diagnóstico de SM, a apresentação cutânea infrequente mereceu os diagnósticos diferenciais agrupados como síndrome verrucosa, em especial a esporotricose.
Downloads
Referências
1. Ghanem KG, Ram S, Rice PA. The Modern Epidemic of Syphilis. N Engl J Med. 2020; 382(9):845-854.
2. Karp G, Schlaeffer F, Jotkowitz A, Riesenberg K. Syphilis and HIV co-infection. Eur J Intern Med. 2009; 20(1):9-13.
3. Zetola NM, Klausner JD. Syphilis and HIV infection: an update. Clin Infect Dis. 2007; 44(9):1222-8.
4. Cid PM, Cudós ES, Zamora Vargas FX, Merino MJ, Pinto PH. Pathologically confirmed malignant syphilis using immunohistochemical staining: report of 3 cases and review of the literature. Sex Transm Dis. 2014; 41(2):94-7.
5. Wibisono O, Idrus I, Djawad K. Sífilis maligna: revisión sistemática de los casos publicados entre los anos 2014-2018. Actas Dermosifiliogr. 2021; 112:725-734.
6. Fisher DA, Chang LW, Tuffanelli DL. Lues maligna: presentation of a case and a review of the literature. Arch Dermatol. 1969; 99(1):70-3.
7. Gregory N, Sanchez M, Buchness MR. The spectrum of syphilis in patients with human immunodeficiency virus infection. J Am Acad Dermatol. 1990; 22:1061-7.
8. Sands M, Markus A. Lues maligna, or ulceronodular syphilis, in a man infected with human immunodeficiency virus: case report and review. Clin Infect Dis. 1995; 20:387-90.
9. Costa PP, Moura AA, Rodrigues FLM, Almeida MP, Vilasboas V, Francesconi F. Sífilis maligna precoce em paciente imunodeprimido. Revista SPDV 2019; 77(2).
10. Rosenheim M, Brucker G, Leibowitch M, Niel G, Bournerias I, Duflo B, et al. Syphilis maligne chez un malade porteur d’anticorps anti-HIV [FRE]. Presse Med. 1987; 16(16):777.
11. Santos TR, Castro IJ, Dahia MM, Azevedo MC, Silva GA, Motta RN, et al. Malignant syphilis in an AIDS patient. Infection. 2015; 43(2):231-6.
12. Costa F, Martinez C, Azulay L. PLECT: enfermedades tropicales de manifestación verrucosa. Rev chil dermatol. 2018; 34(3):89-94.
13. Marra CM, Maxwell CL, Smith SL, Lukehart SA, Rompalo AM, Eaton M,et al. Cerebrospinal fluid abnormalities in patients with syphilis: association with clinical and laboratory features. J Infect Dis. 2004; 189:369-76.
14. Libois A, De Wit S, Poll B, Garcia F, Florence E, Del Rio A, et al. HIV and syphilis: when to perform a lumbar puncture. Sex Transm Dis. 2007; 34(3):141-4.
15. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância, Prevenção e Controle das Infecções Sexualmente Transmissíveis, do HIV/Aids e das Hepatites Virais. Protocolo clínico e diretrizes terapêuticas para manejo da infecção pelo HIV em adultos. Brasília: MS; 2018.
Downloads
Publicado
Como Citar
Edição
Seção
Licença
Copyright (c) 2022 Infectologia em Evidência

Este trabalho está licenciado sob uma licença Creative Commons Attribution 4.0 International License.
Todos os usuários podem ler, baixar, compartilhar e adaptar esta produção científica livremente para quaisquer fins (mesmo que comerciais), desde que seja dado o devido crédito aos autores e à publicação original e que qualquer alteração seja devidamente indicada.
> Ética
Todos os artigos publicados na Revista gozam de uma aprovação ética do Sistema Nacional de Ética em Pesquisa (antigo sistema CEP/CONEP) com base na Lei Federal 14.874/24 e outras regulamentações específicas brasileiras ou documento semelhante atestando a ciência e autorização por parte da instituição de origem no caso de trabalhos estrangeiros.
Os autores declaram não haver nenhum tipo de patrocínio ou conflito de interesses, salvo indicação em contrário no corpo do artigo.
Vale ressaltar que os relatos de caso são um valioso recurso de aprendizado para a comunidade científica, mas não devem ser utilizados isoladamente para guiar opções diagnósticas ou terapêuticas na prática clínica ou em políticas de saúde.








