
Criptococose cutânea: doença sistêmica ou localizada?
DOI:
https://doi.org/10.5935/2764-734X.e20230324Palavras-chave:
Criptococose, Infecções fúngicas invasivas, Manifestações cutâneas, Relato de casoResumo
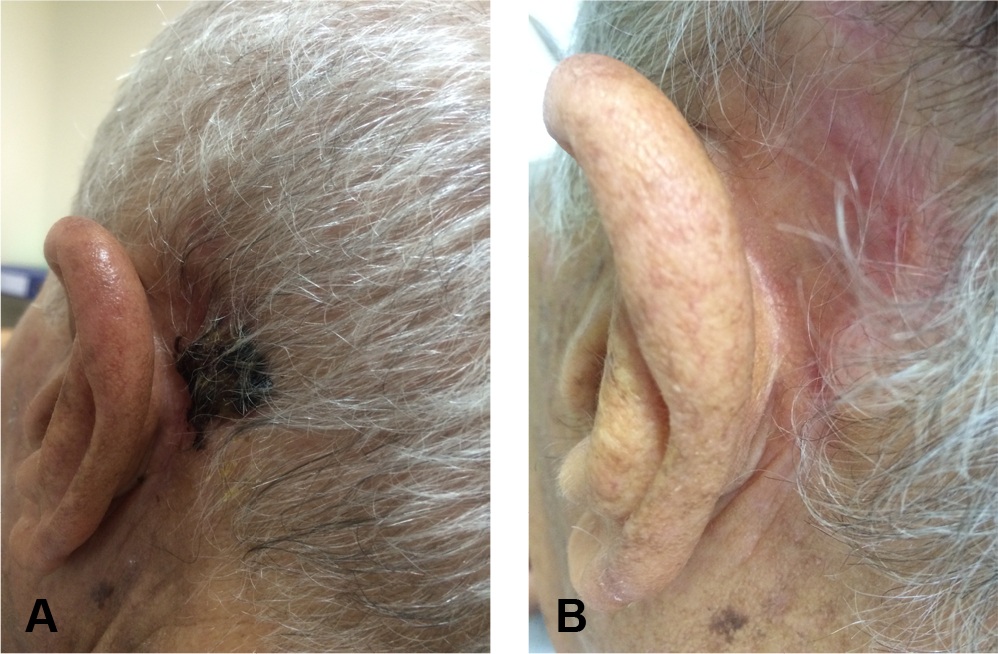
A criptococose cutânea é uma infecção fúngica que pode se manifestar como doença localizada ou disseminada, tanto em pacientes imunocompetentes quanto imunodeprimidos. O presente relato corresponde a um paciente de 81 anos de idade, procedente da zona rural da Bahia, com a forma cutânea da doença. Inicialmente considerado como portador de criptococose primária, foi medicado com fluconazol. A fim de descartar a doença disseminada; entretanto, o paciente foi submetido à tomografia de tórax que evidenciou nódulos pulmonares que, associados à antigenemia positiva, justificaram a mudança para anfotericina B lipossomal. Houve resposta clínica satisfatória, sem aparentes complicações relacionadas ao tratamento, porém o diagnóstico tardio de uma neoplasia de próstata metastática permitiu o questionamento desta suposta disseminação da infecção fúngica. A diferenciação entre criptococose localizada e disseminada nem sempre é fácil, mas é fundamental para o direcionamento adequado do tratamento.
Downloads
Referências
1. Christanson JC, Engber W, Andes D. Primary cutaneous cryptococcosis in immunocompetent and immunocompromised hosts. Med Mycol J. 2003 Jun;41(3):177-88.
2. Du L, Yang Y, Gu J, Chen J, Liao W, Zhu Y. Systemic review of published reports on primary cutaneous cryptococcosis in immunocompetent patients. Mycopathologia. 2015 Aug;180(1-2):19-25.
3. Noguchi H, Matsumoto T, Kimura U, Hiruma M, Kusuhara M, Ihn H. Cutaneous cryptococcosis. Med Mycol J. 2019;60(4):101-7.
4. Marques SA, Bastazini Junior I, Martins AL, Barreto JA, Barbieri D’Elia MP, Lastória JC, et al. Primary cutaneous cryptococcosis in Brazil: report of 11 cases in immunocompetent and immunosuppressed patients. Int J Dermatol. 2012 Jul;51(7):780-4.
5. Ng WF, Loo KT. Cutaneous cryptococcosis – primary versus secondary disease: report of two cases and review of the literature. Am J Dermatopathol. 1993 Aug;15(4):372-7.
6. Tabassum S, Rahman A, Herekar F, Masood S. Cryptococcal meningitis with secondary cutaneous involvement in an immunocompetent host. J Infect Dev Ctries. 2013 Sep;7(9):680-5.
7. Murakawa GJ, Kerschmann R, Berger T. Cutaneous Cryptococcus infection and AIDS: report of 12 cases and review of the literature. Arch Dermatol. 1996 May;132(5):545-8.
8. Pema K, Diaz J, Guerra LG, Nabhan D, Verghese A. Disseminated cryptococcosis: comparison of clinical manifestations in the pre-AIDS and AIDS era. Arch Intern Med. 1994 May;154(9):1032-4.
9. Amaral DM, Rocha RC, Carneiro LE, Vasconcelos DM, Abreu MA. Disseminated cryptococcosis manifested as a single tumor in an immunocompetent patient, similar to the cutaneous primary forms. An Bras Dermatol. 2016 Sep/Oct;91(5 Suppl 1):S29-S31.
10. Mayers DL, Martone WJ, Mandell GL. Cutaneous cryptococcosis mimicking gram-positive cellulitis in a renal transplant patient. South Med J. 1981 Aug;74(8):1032-3.
11. Lima AM, Rodrigues MM, Reis CMS. Cutaneous cryptococcosis mimicking leishmaniasis. Am J Trop Med Hyg. 2018 Jan;98(1):3-4.
12. Moretti ML, Resende MR, Lazéra MS, Colombo AL, Shikanai-Yasuda MA. Consenso em criptococose-2008. Rev Soc Bras Med Trop. 2008;41(5):524-44.
13. Miller Junior WT, Edelman JM, Miller WT. Cryptococcal pulmonary infections in patients with AIDS: radiographic appearance. Radiology. 1990 Jun;175(3):725-8.
14. Setianingrum F, Rautemaa-Richardson R, Denning DW. Pulmonary cryptococcosis: a review of pathobiology and clinical aspects. Med Mycol. 2019;57(2):133-50.
15. Limper AH. The changing spectrum of fungal infections in pulmonary and critical care practice: clinical approach to diagnosis. Proc Am Thorac Soc. 2010;7:163-8.
16. Swinne D, De Vroey C. Detection of circulating capsular polysaccharide antigenfrom Cryptococcus neoformans. J Clin Microbiol. 1992 Sep;30(9):2521.
17. Hafner C, Linde HJ, Vogt T, Breindl G, Tintelnot K, Koellner K, et al. Primary cutaneous cryptococcosis and secondary antigenemia in a patient with long-term corticosteroid therapy. Infection. 2005 Apr;33(2):86-9.
18. Nunez M, Peacock Junior JE, Chin Junior R. Pulmonary cryptococcosis in the immunocompetent host: therapy with oral fluconazole: a report of four cases and a review of the literature. Chest. 2000 Aug;118(2):527-34.
19. Neuville S, Dromer F, Morin O, Dupont B, Ronin O, Lortholary O. Primary cutaneous cryptococcosis: a distinct clinical entity. Clin Infect Dis. 2003 Feb;36(3):337-47.
20. Yamaguchi H, Komase Y, Ikehara M, Yamamoto T, Shinagawa T. Disseminated cryptococcal infection with eosinophilia in a healthy person. J Infect Chemother. 2008 Aug;14(4):319-24.
Downloads
Publicado
Como Citar
Edição
Seção
Licença
Copyright (c) 2023 Infectologia em Evidência

Este trabalho está licenciado sob uma licença Creative Commons Attribution 4.0 International License.
Todos os usuários podem ler, baixar, compartilhar e adaptar esta produção científica livremente para quaisquer fins (mesmo que comerciais), desde que seja dado o devido crédito aos autores e à publicação original e que qualquer alteração seja devidamente indicada.
> Ética
Todos os artigos publicados na Revista gozam de uma aprovação ética do Sistema Nacional de Ética em Pesquisa (antigo sistema CEP/CONEP) com base na Lei Federal 14.874/24 e outras regulamentações específicas brasileiras ou documento semelhante atestando a ciência e autorização por parte da instituição de origem no caso de trabalhos estrangeiros.
Os autores declaram não haver nenhum tipo de patrocínio ou conflito de interesses, salvo indicação em contrário no corpo do artigo.
Vale ressaltar que os relatos de caso são um valioso recurso de aprendizado para a comunidade científica, mas não devem ser utilizados isoladamente para guiar opções diagnósticas ou terapêuticas na prática clínica ou em políticas de saúde.








