
Endocardite por Lactobacillus spp. em paciente imunocompetente
DOI:
https://doi.org/10.5935/2764-734X.e20230829Palavras-chave:
Endocardite bacteriana subaguda, Lactobacillus, Antibióticos, Penicilina, Procedimentos cirúrgicos cardíacos, Relato de casoResumo
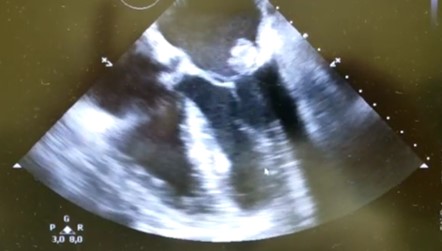
Lactobacillus são bacilos gram-positivos, facultativos ou estritamente anaeróbicos que podem ser comumente encontrados no trato gastrintestinal e no trato genital feminino, sendo patógenos humanos infrequentes. Aqui apresentamos um caso raro de endocardite infecciosa causada por espécie de Lactobacillus em paciente sem imunodeficiência conhecida prévia. Após apresentar quadro febril subagudo e sintomas de insuficiência cardíaca, paciente foi submetido a ecocardiograma, com identificação de vegetação em valva mitral. Hemoculturas coletadas na admissão do paciente resultaram no crescimento de Lactobacillus casei/paracasei/rhamnosus em todas as amostras. A concentração inibitória mínima (CIM) de penicilina para o agente identificado foi de 0,38mg/L. O paciente foi tratado com monoterapia de betalactâmico por seis semanas, associada à remoção cirúrgica eletiva do componente valvar acometido. Evoluiu com boa resposta clínica, sem intercorrências e sem recorrência dos sintomas decorridos 45 dias após a alta hospitalar.
Downloads
Referências
1. Bourne KA, Beebe JL, Lue YA, Ellner PD. Bacteremia due to Bifidobacterium, Eubacterium or Lactobacillus; twenty-one cases and review of the literature. Yale J Biol Med. 1978 Sep/Oct;51(5):505-12.
2. Petrova MI, Lievens E, Malik S, Imholz N, Lebeer S. Lactobacillus species as biomarkers and agents that can promote various aspects of vaginal health. Front Physiol. 2015 Mar;6:81.
3. Alvarez-Olmos MI, Oberhelman RA. Probiotic agents and infectious diseases: a modern perspective on a traditional therapy. Clin Infect Dis. 2001 Jun;32(11):1567-76.
4. Cannon JP, Lee TA, Bolanos JT, Danziger LH. Pathogenic relevance of Lactobacillus: a retrospective review of over 200 cases. Eur J Clin Microbiol Infect Dis. 2005 Jan;24(1):31-40.
5. See JR, Czachor JS, Brown GR. Lactobacillus endocarditis: case report and literature review. Infect Dis Clin Prac. 2006;14(3):134-6.
6. Borriello SP, Hammes WP, Holzapfel W, Marteau P, Schrezenmeir J, Vaara M, et al. Safety of probiotics that contain lactobacilli or bifidobacteria. Clin Infect Dis. 2003 Mar;36(6):775-80.
7. Husni RN, Gordon SM, Washington JA, Longworth DL. Lactobacillus bacteremia and endocarditis: review of 45 cases. Clin Infect Dis. 1997 Nov;25(5):1048-55.
8. Harty DW, Patrikakis M, Hume EB, Oakey HJ, Knox KW. The aggregation of human platelets by Lactobacillus species. J Gen Microbiol. 1993 Dec;139(12):2945-51.
9. Harty DW, Oakey HJ, Patrikakis M, Hume EB, Knox KW. Pathogenic potential of lactobacilli. Int J Food Microbiol. 1994 Dec;24(1-2):179-89.
10. Grazioli-Gauthier L, Rigamonti E, Leo LA, Lucchini GM, Priore EL, Bernasconi E. Lactobacillus jensenii mitral valve endocarditis: case report, literature review and new perspectives. IDCases [Internet]. 2022; 27:e01401. Disponível em: https://www.sciencedirect.com/science/article/pii/ S2214250922000294?via%3Dihub
11. Brouqui P, Raoult D. Endocarditis due to rare and fastidious bacteria. Clin Microbiol Rev. 2001 Jan;14(1):177-207.
12. Bayer AS, Chow AW, Betts D, Guze LB. Lactobacillemia — report of nine cases: Important clinical and therapeutic considerations. Am J Med. 1978 May;64(5):808-13.
13. Griffiths JK, Daly JS, Dodge RA. Two cases of endocarditis due to Lactobacillus species: antimicrobial susceptibility, review, and discussion of therapy. Clin Infect Dis. 1992 Aug;15(2):250-5.
14. Sussman JI, Baron EJ, Goldberg SM, Kaplan MH, Pizzarello RA. Clinical manifestations and therapy of Lactobacillus endocarditis: report of a case and review of the literature. Rev Infect Dis. 1986 Sep/ Oct;8(5):771-6.
15. Lebeaux D, Fernández-Hidalgo N, Pilmis B, Tattevin P, Mainardi JL. Aminoglycosides for infective endocarditis: time to say goodbye?. Clin Microbiol Infec. 2020 Jun;26(6):723-8.
16. Oakey HJ, Harty DW, Knox KW. Enzyme production by lactobacilli and the potential link with infective endocarditis. J Appl Microbiol. 1995 Feb;78(2):142-8.
Downloads
Publicado
Como Citar
Edição
Seção
Licença
Copyright (c) 2023 Infectologia em Evidência

Este trabalho está licenciado sob uma licença Creative Commons Attribution 4.0 International License.
Todos os usuários podem ler, baixar, compartilhar e adaptar esta produção científica livremente para quaisquer fins (mesmo que comerciais), desde que seja dado o devido crédito aos autores e à publicação original e que qualquer alteração seja devidamente indicada.
> Ética
Todos os artigos publicados na Revista gozam de uma aprovação ética do Sistema Nacional de Ética em Pesquisa (antigo sistema CEP/CONEP) com base na Lei Federal 14.874/24 e outras regulamentações específicas brasileiras ou documento semelhante atestando a ciência e autorização por parte da instituição de origem no caso de trabalhos estrangeiros.
Os autores declaram não haver nenhum tipo de patrocínio ou conflito de interesses, salvo indicação em contrário no corpo do artigo.
Vale ressaltar que os relatos de caso são um valioso recurso de aprendizado para a comunidade científica, mas não devem ser utilizados isoladamente para guiar opções diagnósticas ou terapêuticas na prática clínica ou em políticas de saúde.








