
Infecção nosocomial por Cupriavidus metallidurans
DOI:
https://doi.org/10.5935/2764-734X.e20240945Palavras-chave:
Ralstonia, Cupriavidus, Espectrometria de Massa por Dessorção- Ionização de Laser em Matriz, Infecções Nosocomiais;, Relato de CasoResumo
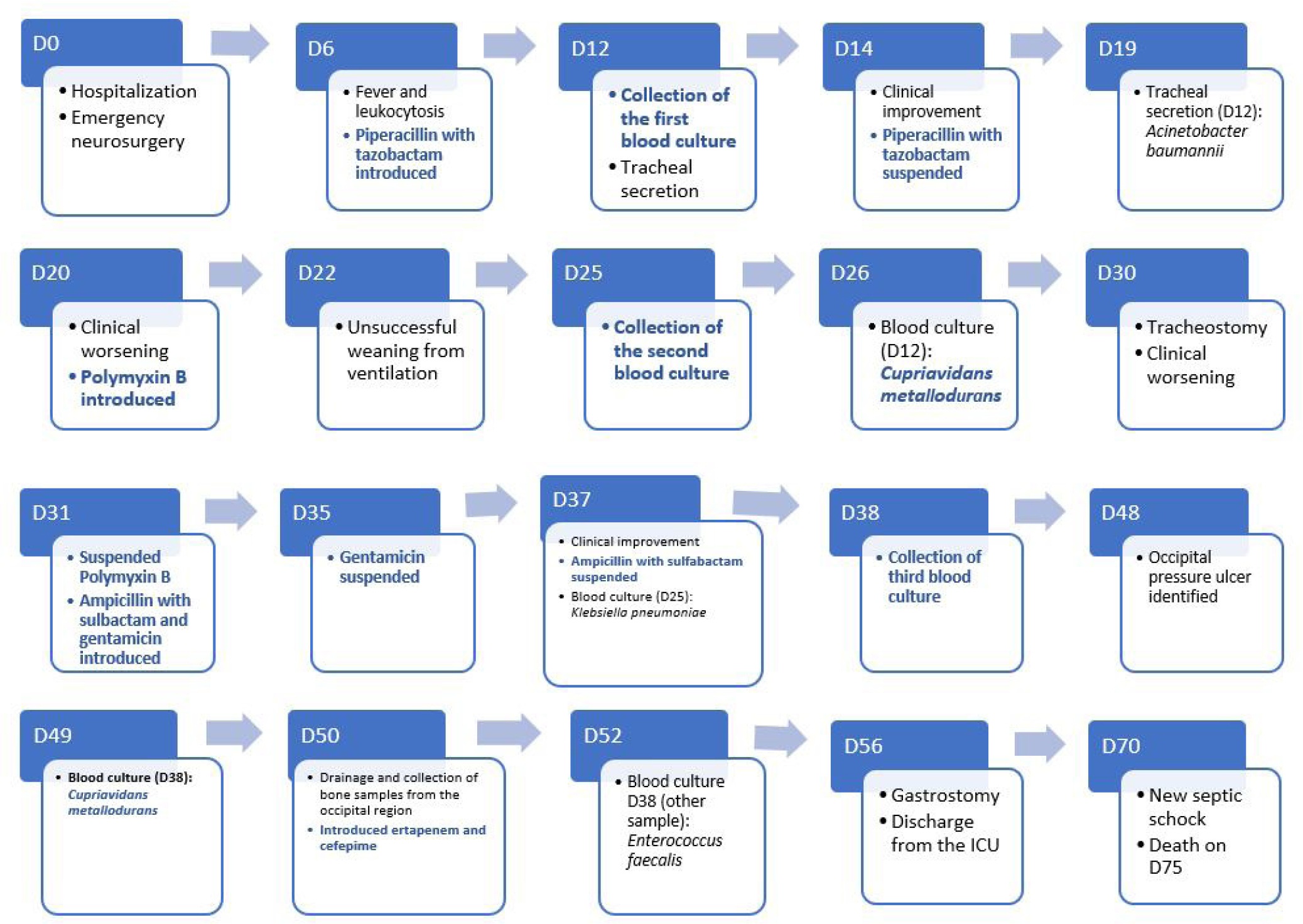
Um paciente masculino de 68 anos permaneceu internado por 75 dias em uma Unidade de Terapia Intensiva após cirurgia para drenagem de hemorragia craniana intraparenquimatosa e colocação de derivação ventricular externa. Durante esta internação prolongada, sua evolução foi complexa, com várias intercorrências e quadros infecciosos de focos variáveis. Nesse contexto, houve crescimento de Cupriavidus metallidurans (identificada pela técnica de MALDI-TOF MS) em duas amostras de hemocultura de sangue periférico, em um intervalo de 26 dias entre as coletas. Além das particularidades desta bactéria raramente isolada no ambiente hospitalar, a revisão deste caso nos incitou a considerar este agente como capaz de provocar infecção ativa, podendo esta ter sido uma possível causa do óbito do paciente.
Downloads
Referências
1. D'Inzeo T, Santangelo R, Fiori B, De Angelis G, Conte V, Giaquinto A, et al. Catheter-related bacteremia by Cupriavidus metallidurans. Diagn Microbiol Infect Dis. 2015 Jan;81(1):9-12. DOI: 10.1016/j.diagmicrobio.2014.09.015
2. Procop G, Church D, Hall G, Janda W, Koneman E, Schreckenberger P. The Nonfermentative Gram-negative Bacilli. In: Koneman's Color Atlas and Textbook of Diagnostic Microbiology. 7th ed. Philadelphia: Wolters Kluwer Health; 2017. p. 797-1059.
3. Notaro A, Vanacore A, Molinaro A, Speciale I. Structure and Conformation Study of the O-Antigen from the Lipopolysaccharide of Cupriavidus metal lidurans CH34. Polysaccharides. 2022; 3(1):188-99. DOI: 10.3390/polysaccharides3010009
4. Falkinham III JO. Introduction to Emerging Opportunistic Premise Plumbing Pathogens. In: Opportunistic Premise Plumbing Pathogens. Singapura: Jenny Stanford Publishing Pte Ltd; 2023. DOI: 10.1201/9781003321002
5. Monsieurs P, Provoost A, Mijnendonckx K, Leys N, Gaudreau C, Van Houdt R. Genome Sequence of Cupriavidus metallidurans Strain H1130, Isolated from an Invasive Human Infection. Genome Announc. 2013;1(6):e01051-13. DOI: 10.1128/genomeA.01051-13
6. Diels L, Van Roy S, Taghavi S, Van Houdt R. From industrial sites to environmental applications with Cupriavidus metallidurans. 2009;96(2):247-58. DOI: 10.1007/s10482-009-9361-4
7. Wauters G, Claeys G, Verschraegen G, De Baere T, Vandecruys E, Van Simaey L, et al. Case of catheter sepsis with Ralstonia gilardii in a child with acute lymphoblastic leukemia. J Clin Microbiol. 2001;39(12):4583-4. DOI: 10.1128/JCM.39.12.4583-4584.2001
8. Karafin M, Romagnoli M, Fink DL, Howard T, Rau R, Milstone AM, et al. Fatal infection caused by Cupriavidus gilardii in a child with aplastic anemia. J Clin Microbiol. 2010;48(3):1005-7. DOI: 10.1128/JCM.01482-09
9. Stovall SH, Wisdom C, McKamie W, Ware W, Dedman H, Fiser RT. Nosocomial transmission of Cupriavidus pauculus during extracorporeal membrane oxygenation. ASAIO J. 2010;56(5):486-7. DOI: 10.1097/MAT.0b013e3181f0c80d
10. Langevin S, Vincelette J, Bekal S, Gaudreau C. First case of invasive human infection caused by Cupriavidus metallidurans. J Clin Microbiol. 2011;49(2):744-5. DOI: 10.1128/JCM.01947-10
11. Santiago AJ, Burgos-Garay ML, Kartforosh L, Mazher M, Donlan RM. Bacteriophage treatment of carbapenemase-producing Klebsiella pneumoniae in a multispecies biofilm: a potential biocontrol strategy for healthcare facilities. AIMS Microbiol. 2020;6(1):43-63. DOI: 10.3934/microbiol.2020003
12. Sohrabi A, Norouzfar ZS, Eslamifar A, Arashkia A, Azadmanesh K. Isolation of Cupriavidus metallidurans from razor blade during paraffin embedded tissue sectioning. Clin Lab. 2011;57(7-8):641
13. Coenye T, Spilker T, Reik R, Vandamme P, Lipuma JJ. Use of PCR analyses to define the distribution of Ralstonia species recovered from patients with cystic fibrosis. J Clin Microbiol. 2005;43(7):3463-6. DOI: 10.1128/JCM.43.7.3463-3466.2005
14. Spilker T, Coenye T, Vandamme P, LiPuma JJ. PCR-based assay for differentiation of Pseudomonas aeruginosa from other Pseudomonas species recovered from cystic fibrosis patients. J Clin Microbiol. 2004;42(5):2074-9. DOI: 10.1128/JCM.42.5.2074-2079.2004
15. Pasternak J. New methods of microbiological identification using MALDI-TOF. Einstein (Sao Paulo). 2012;10(1):118-9. DOI: 10.1590/s1679-45082012000100026
Downloads
Publicado
Como Citar
Edição
Seção
Licença
Copyright (c) 2025 Infectologia em Evidência

Este trabalho está licenciado sob uma licença Creative Commons Attribution 4.0 International License.
Todos os usuários podem ler, baixar, compartilhar e adaptar esta produção científica livremente para quaisquer fins (mesmo que comerciais), desde que seja dado o devido crédito aos autores e à publicação original e que qualquer alteração seja devidamente indicada.
> Ética
Todos os artigos publicados na Revista gozam de uma aprovação ética do Sistema Nacional de Ética em Pesquisa (antigo sistema CEP/CONEP) com base na Lei Federal 14.874/24 e outras regulamentações específicas brasileiras ou documento semelhante atestando a ciência e autorização por parte da instituição de origem no caso de trabalhos estrangeiros.
Os autores declaram não haver nenhum tipo de patrocínio ou conflito de interesses, salvo indicação em contrário no corpo do artigo.
Vale ressaltar que os relatos de caso são um valioso recurso de aprendizado para a comunidade científica, mas não devem ser utilizados isoladamente para guiar opções diagnósticas ou terapêuticas na prática clínica ou em políticas de saúde.








