
Disfunção hipofisária associada a meningite tuberculosa
DOI:
https://doi.org/10.5935/2764-734X.e20250462Palavras-chave:
Tuberculose endócrina, Tuberculose do Sistema Nervoso Central, Hipofisite, Relato de casoResumo
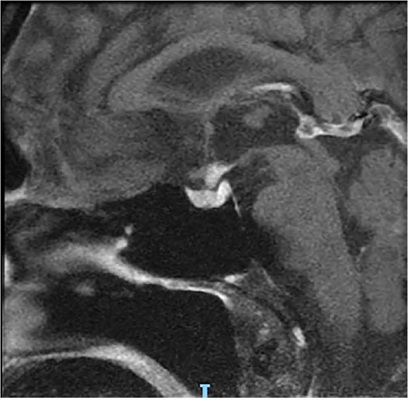
A tuberculose pode cursar com alterações endócrino-metabólicas em diferentes glândulas com apresentação e formas clínicas variadas, sendo que a incidência do acometimento da hipófise é desconhecida. Apresentamos um caso de paciente com diagnóstico recente de aids que, ao apresentar meningite tuberculosa, cursou com diabetes insipidus, hipogonadismo hipogonadotrófico e hiperprolactinemia. O diagnóstico de hipofisite ficou bem estabelecido, no entanto não houve recuperação total da função hormonal mesmo após o tratamento específico.
Downloads
Referências
1. Vinnard C, Blumberg EA. Endocrine and Metabolic Aspects of Tuberculosis. Microbiol Spectr. 2017 Jan;5(1):10.1128/microbiolspec.tnmi7-0035-2016. DOI: 10.1128/microbiolspec.tnmi7-0035-2016
2. Beatrice AM, Selvan C, Mukhopadhyay S. Pituitary dysfunction in infective brain diseases. Indian J Endocrinol Metab. 2013 Dec;17(Suppl 3):S608-11. DOI: 10.4103/2230-8210.123546
3. Lam KS, Sham MM, Tam SC, Ng MM, Ma HT. Hypopituitarism after tuberculous meningitis in childhood. Ann Intern Med. 1993 May 1;118(9):701-6. DOI: 10.7326/0003-4819-118-9-199305010-00007
4. Dhanwal DK, Vyas A, Sharma A, Saxena A. Hypothalamic pituitary abnormalities in tubercular meningitis at the time of diagnosis. Pituitary. 2010 Dec;13(4):304-10. DOI: 10.1007/s11102-010-0234-7
5. Ranjan A, Chandy MJ. Intrasellar tuberculoma. Br J Neurosurg. 1994;8(2):179-85. DOI: 10.3109/02688699409027964
6. Cherian A, Ajitha KC, Iype T, Divya KP. Neurotuberculosis: an update. Acta Neurol Belg. 2021 Feb;121(1):11-21. DOI: 10.1007/s13760-020-01575-0
7. Correia-Neves M, Fröberg G, Korshun L, Viegas S, Vaz P, Ramanlal N, et al. Biomarkers for tuberculosis: the case for lipoarabinomannan. Biomarkers for tuberculosis: the case for lipoarabinomannan. ERJ Open Res. 2019 Feb 11;5(1):00115-2018. DOI: 10.1183/23120541.00115-2018
8. Schaller MA, Wicke F, Foerch C, Weidauer S. Central Nervous System Tuberculosis: Etiology, Clinical Manifestations and Neuroradiological Features. Clin Neuroradiol. 2019 Mar;29(1):3-18. DOI: 10.1007/s00062-018-0726-9
9. Siddiqi OK, Birbeck GL, Ghebremichael M, Mubanga E, Love S, Buback C, et al. Prospective Cohort Study on Performance of Cerebrospinal Fluid (CSF) Xpert MTB/RIF, CSF Lipoarabinomannan (LAM) Lateral Flow Assay (LFA), and Urine LAM LFA for Diagnosis of Tuberculous Meningitis in Zambia. J Clin Microbiol. 2019 Jul 26;57(8):e00652-19. DOI: 10.1128/JCM.00652-19
10. Sulaiman T, Medi S, Erdem H, Senbayrak S, Ozturk-Engin D, Inan A, et al. The diagnostic utility of the “Thwaites’ system” and “lancet consensus scoring system” in tuberculous vs. non-tuberculous subacute and chronic meningitis: multicenter analysis of 395 adult patients. BMC Infect Dis. 2020 Oct 23;20(1):788. DOI: 10.1186/s12879-020-05502-9
11. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Manual de recomendações para o controle da tuberculose no Brasil. 2a ed. Brasília: Ministério da Saúde; 2019 [acesso 2025 fev 20]. Disponível em: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/svsa/tuberculose/manual-de-recomendacoes-e-controle-da-tuberculose-no-brasil-2a-ed.pdf/view
12. Brasil. Ministério da Saúde. Secretaria de Ciência, Tecnologia, Inovação e Complexo da Saúde. Secretaria de Vigilância em Saúde e Ambiente. Protocolo Clínico e Diretrizes Terapêuticas para Manejo da Infecção pelo HIV em Adultos: Módulo 2: Coinfecções e Infecções Oportunistas [recurso eletrônico]. Brasília: Ministério da Saúde; 2023 [acesso 2025 fev 20]. Disponível em: https://www.gov.br/aids/pt-br/central-de-conteudo/pcdts/PCDT_HIV_Modulo_2_2024_eletrnicoISBN.pdf
13. Delsedime M, Aguggia M, Cantello R, Chiado Cutin I, Nicola G, Torta R, et al. Isolated hypophyseal tuberculoma: case report. Clin Neuropathol. 1988 Nov/Dec;7(6):311-3.
14. Srisukh S, Tanpaibule T, Kiertiburanakul S, Boongird A, Wattanatranon D, Panyaping T, et al. Pituitary tuberculoma: A consideration in the differential diagnosis in a patient manifesting with pituitary apoplexy-like syndrome. IDCases. 2016 Jul 29;5:63-6. DOI: 10.1016/j.idcr.2016.07.012
15. Tanimoto K, Imbe A, Shishikura K, Imbe H, Hiraiwa T, Miyata T, et al. Reversible hypopituitarism with pituitary tuberculoma. Intern Med. 2015;54(10):1247-51. DOI: 10.2169/internalmedicine.54.3435
Downloads
Publicado
Como Citar
Edição
Seção
Licença
Copyright (c) 2025 Infectologia em Evidência

Este trabalho está licenciado sob uma licença Creative Commons Attribution 4.0 International License.
Todos os usuários podem ler, baixar, compartilhar e adaptar esta produção científica livremente para quaisquer fins (mesmo que comerciais), desde que seja dado o devido crédito aos autores e à publicação original e que qualquer alteração seja devidamente indicada.
> Ética
Todos os artigos publicados na Revista gozam de uma aprovação ética do Sistema Nacional de Ética em Pesquisa (antigo sistema CEP/CONEP) com base na Lei Federal 14.874/24 e outras regulamentações específicas brasileiras ou documento semelhante atestando a ciência e autorização por parte da instituição de origem no caso de trabalhos estrangeiros.
Os autores declaram não haver nenhum tipo de patrocínio ou conflito de interesses, salvo indicação em contrário no corpo do artigo.
Vale ressaltar que os relatos de caso são um valioso recurso de aprendizado para a comunidade científica, mas não devem ser utilizados isoladamente para guiar opções diagnósticas ou terapêuticas na prática clínica ou em políticas de saúde.








