
Infecção por Mycobacterium abscessus após procedimento cirúrgico estético
DOI:
https://doi.org/10.5935/2764-734X.e20231030Palavras-chave:
Mycobacterium abscessus, Infecções por Mycobacterium não tuberculosas, Complicações pós-operatórias, Procedimentos cirúrgicos estéticos, Relato de casoResumo
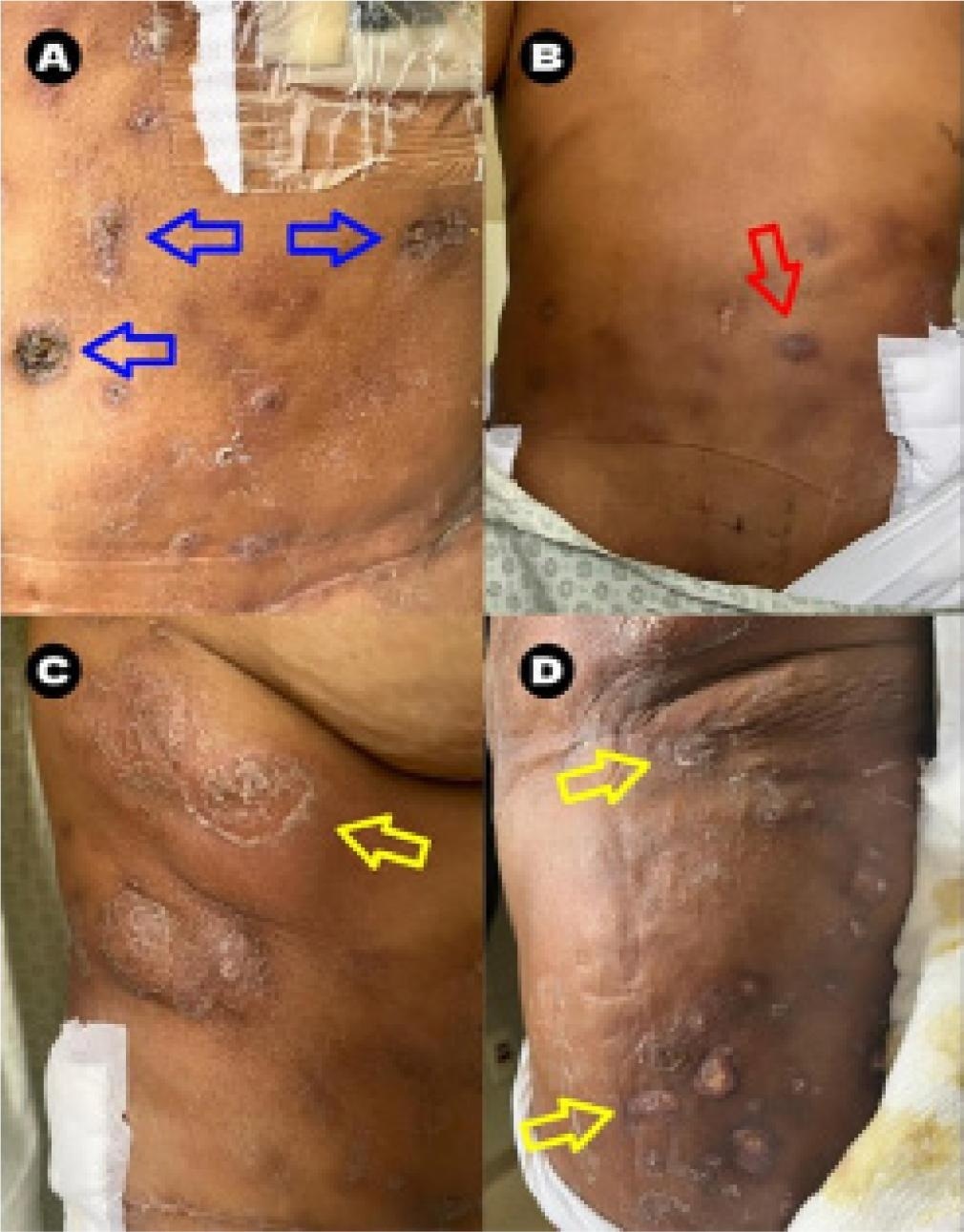
A infecção por Mycobacterium abscessus é incomum, contudo o aumento de casos tem sido relatado de forma emergente, sobretudo quando associado a traumas e infecções relacionadas à assistência à saúde após procedimentos cirúrgicos estéticos. Muitas vezes a infecção é de difícil diagnóstico e com indicação de tratamento prolongado, apresentando baixa mortalidade, mas importante morbidade ao paciente. Este relato descreve um caso de infecção por Mycobacterium abscessus com manifestação miocutânea após lipoaspiração abdominal e enxerto glúteo, manifestada por lesões úlcero-crostosas difusas, coleções subcutâneas e miofasciais, fasciite e sintomas constitucionais. O diagnóstico foi obtido pela cultura específica de secreção profunda. Foi iniciado tratamento com amicacina, tigeciclina, claritromicina e ertapenem e manutenção com amicacina, claritromicina e clofazimina que permitiu a regressão das lesões, não obstante prejuízo psicológico e estético.
Downloads
Referências
1. Lyon S, Moura ACL, Grossi MAF, Silva, RCV. Micobacterioses. In: Dermatologia tropical. 1ª ed. Rio de Janeiro: Medbook Editora Científica; 2017. p. 38-41.
2. Nogueira LB, Garcia CN, Costa MSCD, Moraes MB, Kurizky PS, Gomes CM. Non-tuberculous cutaneous mycobacterioses. An Bras Dermatol. 2021;96(5):527-38.
3. Ministério da Saúde (BR). Agência Nacional de Vigilância Sanitária (Anvisa). Boletim Segurança do Paciente e Qualidade em Serviço de Saúde no 19 GVIMS/GGTES/Anvisa: Notificação de casos de micobactéria de crescimento rápido (MCR) atualizado - 1998 a 25 de julho de 2023. Brasília (DF): Ministério da Saúde; 2023; [acesso em 2023 Abr 02]. Disponível em: https://app.powerbi.com/view?r=eyJrIjoiYWU2MTQ3OWItZjAwMy00ZTNkLTk2NzAtMzExMjM0ODc5M2Y0IiwidCI6ImI2N2FmMjNmLWMzZjMtNGQzNS04MGM3LWI3MDg1ZjVlZGQ4MSJ9
4. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis. Recomendações para o diagnóstico e tratamento das doenças causadas por micobactérias não tuberculosas no Brasil. Brasília (DF): Ministério da Saúde; 2021; [acesso em 2023 Abr 02]. Disponível em: https://www.gov.br/aids/pt-br/central-de-conteudo/publicacoes/2021/recomendacoes-para-o-diagnostico-e-tratamento-das-doencas-causadas-por-micobacterias-nao-tuberculosas-no-brasil
5. Sousa PP, Cruz RCS, Schettini APM, Westpha DC. Mycobacterium abscessus skin infection after tattooing - case report. An Bras Dermatol. 2015;90:739-41.
6. Ryu HJ, Kim WJ, Oh CH, Song HJ. Iatrogenic Mycobacterium abscessus infection associated with acupuncture: clinical manifestations and its treatment. Int J Dermatol. 2005;44:846-50.
7. Fitzgerald DA, Smith AG, Lees A, Yee L, Cooper N, Harris SC, et al. Cutaneous infection with Mycobacterium abscessus. Br J Dermatol. 1995;132(5):800-4.
8. Fang RY, Sun QN. Mycobacterium abscessus infections following injection of botulinum toxin. J Cosmet Dermatol. 2020;19(4):817-9.
9. Johansen MD, Herrmann JL, Kremer L. Non-tuberculous mycobacteria and the rise of Mycobacterium abscessus. Nat Rev Microbiol. 2020;18:392-407.
10. Boudehen YM, Kremer L. Mycobacterium abscessus. Trends Microbiol. 2021;29:951-2.
11. Victoria L, Gupta A, Gómez JL, Robledo J. Mycobacterium abscessus complex: a review of recent developments in an emerging pathogen. Front Cell Infect Microbiol. 2021;11:659997.
12. Carvalho NFG, Ferrazoli L, Riveron MBA, Chimara E. Caracterização dos surtos causados pelo grupo Mycobacterium abscessus. Rev Inst Adolfo Lutz. 2012;71(2):228-36.
13. Fröberg G, Maurer FP, Chryssanthou E, Fernström L, Benmansour H, Boarbi S, et al; EUCAST AMST and ESCMYC study groups. Towards clinical breakpoints for non-tuberculous mycobacteria - Determination of epidemiological cut off values for the Mycobacterium avium complex and Mycobacterium abscessus using broth microdilution. Clin Microbiol Infect. 2023 Jun;29(6):758-64.
Downloads
Publicado
Como Citar
Edição
Seção
Licença
Copyright (c) 2023 Infectologia em Evidência

Este trabalho está licenciado sob uma licença Creative Commons Attribution 4.0 International License.
Todos os usuários podem ler, baixar, compartilhar e adaptar esta produção científica livremente para quaisquer fins (mesmo que comerciais), desde que seja dado o devido crédito aos autores e à publicação original e que qualquer alteração seja devidamente indicada.
> Ética
Todos os artigos publicados na Revista gozam de uma aprovação ética do Sistema Nacional de Ética em Pesquisa (antigo sistema CEP/CONEP) com base na Lei Federal 14.874/24 e outras regulamentações específicas brasileiras ou documento semelhante atestando a ciência e autorização por parte da instituição de origem no caso de trabalhos estrangeiros.
Os autores declaram não haver nenhum tipo de patrocínio ou conflito de interesses, salvo indicação em contrário no corpo do artigo.
Vale ressaltar que os relatos de caso são um valioso recurso de aprendizado para a comunidade científica, mas não devem ser utilizados isoladamente para guiar opções diagnósticas ou terapêuticas na prática clínica ou em políticas de saúde.








