
Gnathostomiasis and cutaneous leishmaniasis: a possible co-infection
DOI:
https://doi.org/10.5935/2764-734X.e202203009Keywords:
Leishmaniasis, Cutaneous, Helminths, Skin UlcerAbstract
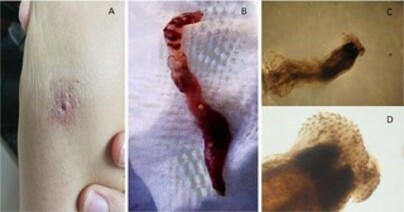
Gnathostomiasis is a zoonosis transmitted to humans by eating raw or undercooked foods contaminated with the larvae of Gnathostoma sp. The clinical manifestations of gnathostomiasis vary according to the species, parasite load and affected tissues. Skin lesions are mainly characterized by nodules or areas of edema that affect any topography of the body. Cutaneous leishmaniasis is mainly characterized by a single ulcerated skin lesion caused by different species of Leishmania. In this article we present a case report of Gnasthostoma and Leishmania co-infection, with clinical presentation of an ulcerated skin lesion in the triceps region of the right upper limb that appeared during a trip to Peru. A diagnosis of leishmaniasis was made by detection of amastigotes and at the beginning of treatment, there was an exit of helminth characterized with Gnasthostoma by stereomicroscope. He received treatment with albendazole, and the lesion healed. This is the first report of Gnasthostoma and Leishmania co-infection described in the literature.
Downloads
References
1. Herman JS, Chiodini PL. Gnathostomiasis, another emerging imported disease. Clin Microbiol Rev. 2009 Jul;22(3):484-92.
2. Peláez D, Pérez-Reyes R. Gnathostomiasis in America. Rev Latinoam Microbiol. 1970 Abr/Jun;12(2):83-91.
3. Ollague W, Ollague J, Guevara de Veliz A, Herrera S. Human gnathostomiasis in Ecuador (nodular migratory eosinophilic panniculitis). First finding of the parasite in South America. Int J Dermatol. 1984 Dez;23(10):647-51.
4. Villar de Cipriani E. Paniculitis migratoria eosinofílica en el Perú: Gnathostoma como agente causal. Rev Peru Med Exp Salud Publica. 2003 Out/Dez;20(4):220-2.
5. Dani CMC, Mota KF, Sanchotene PV, Maceira JP, Maia CPA. Gnatostomíase no Brasil: relato de caso. An Bras Dermatol [Internet]. 2009 Ago; [citado 2021 Feb 8]; 84(4):400-4. Disponível em: https://www.scielo.br/j/abd/a/fc7GmYgcBXnDbx3vZ58bLyN/?lang=pt
6. Vargas TJS, Kahler S, Dib C, Cavaliere MB, Jeunon-Sousa MA. Autochthonous gnathostomiasis, Brazil. Emerg Infect Dis. 2012 Dez;18(12):2087-9.
7. Haddad Junior V, Oliveira ÍF, Bicudo NP, Marques MEA. Gnathostomiasis acquired after consumption of raw fresh water fish in the Amazon region: are port of two cases in Brazil. Rev Soc Bras Med Trop. 2021;54:e20200127.
8. Diaz JH. Gnathostomiasis: an emerging infection of raw fish consumers in Gnathostoma nematode-endemic and nonendemic countries. J Travel Med. 2015 Set/Out;22(5):318-24.
9. Liu G H, Sun MM, Elsheikha HM, Fu YT, Sugiyama H, Ando K, et al. Human gnathostomiasis: a neglected food-borne zoonosis. Parasit Vectors. 2020 Dez;13(1):616.
10. Bravo F, Gontijo B. Gnathostomiasis: an emerging infectious disease relevant to all dermatologists. Ann Bras Dermatol. 2018 Mar;93(2):172-80.
11. Goto H, Lindoso JAL. Cutaneous and mucocutaneous leishmaniasis. Infect Dis Clin North Am. 2012 Jun;26(2):293-307. DOI: https://doi.org/10.1016/j.idc.2012.03.001
12. Leroy J, Cornu M, Deleplancque AS, Loridant S, Dutoit E, Sendid B. Sushi, ceviche and gnathostomiasis - a case report and review of imported infections. Travel Med Infect Dis. 2017 Nov/Dez;20:26-30.
13. Nawa Y, Mallewong W, Intapan PM, Camacho SPD. Gnathostoma. In: Xiao L, Ryan U, Feng Y, eds. Biology of foodborne parasites. Boca Raton: CRC Press; 2015. p. 420-41.
14. Pavli A, Maltezou HC. Leishmaniasis, an emerging infection in travelers. IntJ Infect Dis. 2010 Dez;14(12):e1032-9.
15. Scott P, Novais FO. Cutaneous leishmaniasis: immune responses in protection and pathogenesis. Nat Rev Immunol. 2016 Jul;16(9):581-92.
16. Moreau E, Chauvin A. Immunity against helminths: interactions with the host and the intercurrent infections. J Biomed Biotechnol. 2010;2010:428593.
17. Kraivichian K, Nuchprayoon S, Sitichalernchai P, Chaicumpa W, Yentakam S. Treatment of cutaneous gnathostomiasis with ivermectin. Am J Trop Med Hyg. 2004 Nov;71(5):623-8.
Published
How to Cite
Issue
Section
License
Copyright (c) 2022 Infections in Evidence

This work is licensed under a Creative Commons Attribution 4.0 International License.
All users may freely read, download, share, and adapt this scientific product for any purpose (even commercial ones), provided that due credit is given to the authors and the original publication, and that any alterations are duly indicated.
> Ethics
All articles published herein have received ethical approval from the National Research Ethics System (formerly CEP/CONEP system) based on Federal Law 14.874/24 and other specific Brazilian regulations, or a similar document attesting to the knowledge and authorization from the institution of origin in the case of foreign works.
The authors declare that there is no sponsorship or conflict of interest of any kind, unless otherwise indicated in the body of the article.
It is worth noting that case reports are a valuable learning resource for the scientific community, but should not be used in isolation to guide diagnostic or therapeutic options in clinical practice or health policies








