
Severe malaria with encephalopathy and acute kidney failure
DOI:
https://doi.org/10.5935/2764-734X.e202204013Keywords:
Malaria, Acute kidney injury, Acute febrile encephalopathy, Time-to-treatment, Case ReportAbstract
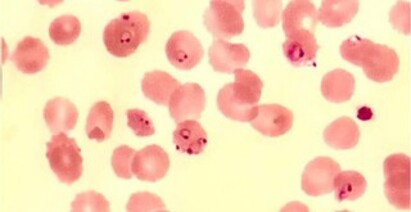
The Legal Amazon region concentrates 99% of malaria cases in Brazil, where Plasmodium vivax is the main etiological agent (90% of cases). This report aims to demonstrate the main role of the patient’s epidemiological history in an acute febrile jaundice syndrome - it’s a case of malaria diagnosed in a patient coming from Benin, Africa, where all cases correspond to Plasmodium falciparum infection. The diagnosis and introduction of appropriate treatment with artesunate were delayed, in such a way that the patient progressed to severe forms of the disease (acute kidney injury and encephalopathy), followed by death.
Downloads
References
1. World Health Organitazion (WHO). World malaria report 2019 [Internet]. Geneva: WHO; 2019. [acesso em 2021 Set 05]. Disponível em: https://www.who.int/publications/i/item/9789241565721
2. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância Epidemiológica. Guia prático de tratamento da malária no Brasil. Brasília (DF): Ministério da Saúde; 2020. [acesso em 2021 Set 05]. Disponível em: https://bvsms.saude.gov.br/bvs/publicacoes/guia_tratamento_malaria_brasil.pdf
3. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Manual de vigilância, prevenção e controle de zoonoses. Brasília (DF): Ministério da Saúde; 2016. [acesso em 2021 Set 05]. Disponível em: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/publicacoes-svs/zoonose/manual-zoonoses-normas-2v-7julho16-site.pdf/view
4. Ministério da Saúde (BR). DATASUS - Indicadores de dados básicos Brasil: índice parasitário anual (IPA) de malária [Internet]. Brasília (DF): Ministério da Saúde; 2021; [acesso em 2020 Set 07]. Disponível em: http://tabnet.datasus.gov.br/cgi/idb2000/fqd04.htm#:~:text=Esse%20risco%20est%C3%A1%20relacionado%20%C3%A0,(%E2%89%A550%2C0)
5. Koopmans L, Wolfswinkel M, Hesselink, D, Hoorn E, Koelewijn R, Van Hellemond JJ, et al. Acute kidney injury in imported Plasmodium falciparum malaria. Malaria J. 2015;14:523. doi: 10.1186/s12936-015-1057-9.
6. Nguansangiam S, Day NPJ, Hien TT, Mai NTH, Chaisri U, Riganti M, et al. A quantitative ultrastructural study of renal pathology in fatal Plasmodium falciparum malaria. Trop Med Int Health. 2007 Set;12(9):1037-50.
7. Mishra SK, Das BS. Malaria and acute kidney injury. Semin Nephrol. 2008 Jul;28(4):395-408.
8. Plewes K, Royakkers AA, Hanson J, Hasan MMU, Alam S, Ghose A, et al. Correlation of biomarkers for parasite burden and immune activation with acute kidney injury in severe falciparum malaria. Malaria J. 2014 Mar;13:91. doi: 10.1186/1475-2875-13-91.
9. Mishra SK, Newton CRJC. Diagnosis and management of the neurological complications of falciparum malaria. Nat Rev Neurol. 2009 Abr;5(4):189-98.
10. Queiroz NL, Teixeira MM, Teixeira AL. Imunopatogênese da malaria cerebral. Rev Bras Neurol. 2008;44(1):13-9.
11. World Health Organitazion (WHO). Severe malaria. Trop Med Int Health. 2014 Set;19(Supl 1):S7-S131. doi: 10.1111/tmi.12313_2.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2022 Infections in Evidence

This work is licensed under a Creative Commons Attribution 4.0 International License.
All users may freely read, download, share, and adapt this scientific product for any purpose (even commercial ones), provided that due credit is given to the authors and the original publication, and that any alterations are duly indicated.
> Ethics
All articles published herein have received ethical approval from the National Research Ethics System (formerly CEP/CONEP system) based on Federal Law 14.874/24 and other specific Brazilian regulations, or a similar document attesting to the knowledge and authorization from the institution of origin in the case of foreign works.
The authors declare that there is no sponsorship or conflict of interest of any kind, unless otherwise indicated in the body of the article.
It is worth noting that case reports are a valuable learning resource for the scientific community, but should not be used in isolation to guide diagnostic or therapeutic options in clinical practice or health policies








