
Oral doxycycline as an alternative treatment for early neurosyphilis in a patient living with HIV
DOI:
https://doi.org/10.5935/2764-734X.e20240947Keywords:
Neurosyphilis, HIV infections, Doxycycline, Case reportAbstract
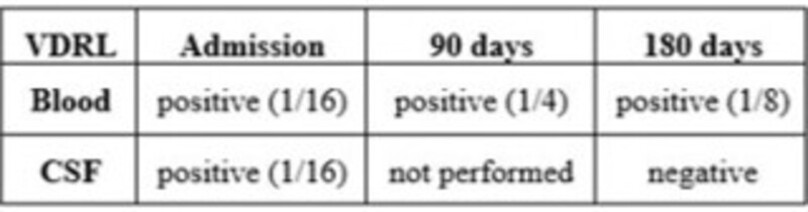
This report aims to describe the successful treatment using oral doxycycline for early neurosyphilis in a patient living with HIV, primarily presenting with skin lesions. The therapeutic proposal, chosen by the patient and based on UK medical guidelines, has not yet been validated by the Brazilian Ministry of Health. The treatment consisted of a single dose of penicillin G benzathine (2.4 million units) administered intramuscularly, followed by oral doxycycline (200 mg twice a day) for 28 days, with quarterly outpatient follow-up. The patient's symptoms resolved on the first visit, and the nontreponemal test (VDRL) in the cerebrospinal fluid was negative after 6 months. The current literature offers inconclusive results; however, this case suggests that oral doxycycline is a safe alternative for treating neurosyphilis in select cases, especially for patients with penicillin allergies, while providing the advantage of avoiding hospitalization.
Downloads
References
1. Avelleira JCR, Bottino G. Sífilis: diagnóstico, tratamento e controle. An Bras Dermatol. 2006;81(2):111-26. DOI: 10.1590/S0365-05962006000200002
2. Chan DJ. Syphilis and HIV co-infection: when is lumbar puncture indicated? Curr HIV Res. 2005;3(1):95-8. DOI: 10.2174/1570162052773031
3. Ceccarelli G, Borrazzo C, Lazzaro A, Innocenti GP, Celani L, Cavallari EN, et al. Diagnostic Issues of Asymptomatic Neurosyphilis in HIV-Positive Patients: A Retrospective Study. Brain Sci. 2019;9(10):278. DOI: 10.3390/brainsci9100278
4. Girometti N, Junejo MH, Nugent D, McOwan A, Whitlock G; 56 Dean Street Collaborative Group. Clinical and serological outcomes in patients treated with oral doxycycline for early neurosyphilis. J Antimicrob Chemother. 2021;76(7):1916-9. DOI: 10.1093/jac/dkab100
5. Janier M, Unemo M, Dupin N, Tiplica GS, Potočnik M, Patel R. 2020 European guideline on the management of syphilis. J Eur Acad Dermatol Venereol. 2021;35(3):574-88. DOI: 10.1111/jdv.16946
6. Brasil. Ministério da Saúde. Protocolo Clínico e Diretrizes para Atenção Integral às Pessoas com Infecções Sexualmente Transmissíveis [Internet]. Brasília: Ministério da Saúde; 2022; [Accessed in 2024 June 23]. Available from: http://antigo.aids.gov.br/pt-br/pub/2022/protocolo-clinico-e-diretrizes-terapeuticas-para-atencao-integral-pessoas-com-infeccoes
7. Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1-187. DOI: 10.15585/mmwr.rr7004a1
8. Kingston M, French P, Higgins S, McQuillan O, Sukthankar A, Stott C, et al. UK national guidelines on the management of syphilis 2015. Int J STD AIDS. 2016;27(6):421-46. DOI: 10.1177/0956462415624059
9. Qin J, Yang T, Wang H, Feng T, Liu X. Potential Predictors for Serofast State after Treatment among HIV-Negative Persons with Syphilis in China: A Systematic Review and Meta-Analysis. Iran J Public Health. 2015;44(2):155-69.
10. Li J, Zheng HY. Early syphilis: serological treatment response to doxycycline/tetracycline versus benzathine penicillin. J Infect Dev Ctries. 2014;8(2):228-32. DOI: 10.3855/jidc.3013
11. Peyriere H, Makinson A, Marchandin H, Reynes J. Doxycycline in the management of sexually transmitted infections. J Antimicrob Chemother. 2018;73(3):553-63. DOI: 10.1093/jac/dkx420
12. Lewis DA, Lukehart SA. Antimicrobial resistance in Neisseria gonorrhoeae and Treponema pallidum: evolution, therapeutic challenges and the need to strengthen global surveillance. Sex Transm Infect. 2011;87(Suppl 2):ii39-43. DOI: 10.1136/sti.2010.047712
13. Araujo RS, Souza ASS, Braga JU. Who was affected by the shortage of penicillin for syphilis in Rio de Janeiro, 2013-2017? Rev Saude Publica. 2020;54:109. DOI: 10.11606/s1518-8787.2020054002196
14. Bettuzzi T, Jourdes A, Robineau O, Alcaraz I, Manda V, Molina JM, et al. Ceftriaxone compared with benzylpenicillin in the treatment of neurosyphilis in France: a retrospective multicentre study. Lancet Infect Dis. 2021;21(10):1441-7. DOI: 10.1016/S1473-3099(20)30857-4
15. Clement ME, Okeke NL, Hicks CB. Treatment of Syphilis. JAMA. 2014;312(18):1905-17. DOI: 10.1001/jama.2014.13259
16. Ghanem KG, Erbelding EJ, Cheng WW, Rompalo AM. Doxycycline compared with benzathine penicillin for the treatment of early syphilis. Clin Infect Dis. 2006;42(6):e45-9. DOI: 10.1086/500406
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2025 Infections in Evidence

This work is licensed under a Creative Commons Attribution 4.0 International License.
All users may freely read, download, share, and adapt this scientific product for any purpose (even commercial ones), provided that due credit is given to the authors and the original publication, and that any alterations are duly indicated.
> Ethics
All articles published herein have received ethical approval from the National Research Ethics System (formerly CEP/CONEP system) based on Federal Law 14.874/24 and other specific Brazilian regulations, or a similar document attesting to the knowledge and authorization from the institution of origin in the case of foreign works.
The authors declare that there is no sponsorship or conflict of interest of any kind, unless otherwise indicated in the body of the article.
It is worth noting that case reports are a valuable learning resource for the scientific community, but should not be used in isolation to guide diagnostic or therapeutic options in clinical practice or health policies








